
Instructions for Use and Controller Operator's Manual
Gebruiksaanwijzing en handleiding voor de regelaar
Mode d'emploi et manuel de l'opérateur du contrôleur
Gebrauchsanweisung und Betriebshandbuch für den Controller
Istruzioni per l'uso e manuale operativo del controller
MAN-07901-4270 Rev. 001
04/2022
Federal Law (USA) restricts this device to sale by or on the order of
a physician with appropriate training.
Krachtens de federale wetgeving (VS) mag dit toestel slechts worden verkocht door of in opdracht
van een arts met de juiste training voor de bediening van dit apparaat.
En vertu de la loi fédérale des États-Unis, ce dispositif ne peut être vendu que par un médecin
ou sur ordonnance médicale.
Laut US-Bundesgesetz darf dieses Produkt nur von einem Arzt oder im Auftrag eines Arztes mit
entsprechender Schulung erworben werden.
La legge federale statunitense limita la vendita di questo dispositivo ai medici dotati di adeguata
preparazione o su prescrizione degli stessi.

1
ENGLISH
CAUTION: FEDERAL (USA) LAW RESTRICTS THIS DEVICE TO
SALE BY OR ON THE ORDER OF A PHYSICIAN TRAINED IN THE
USE OF THE DEVICE.
Read all instructions, cautions and warnings prior to use. Failure
to follow any instructions or to heed any warnings or precautions
could result in serious patient injury.
NOTE: The manual that accompanied the disposable device may
contain a more recent revision of the NovaSuresystem instructions
than the manual provided with the controller.
The NovaSuredisposable device is not to be used with other
controllers and/or RF generators, and the NovaSureRFcontroller is
not to be used with other disposable devices.
The NovaSure disposable device does not contain latex.
Physician Checklist
The physician must:
• have sufficient experience in performing procedures within the uterine
cavity, such as IUD insertion or dilation and curettage (D&C) and with
adequate training, knowledge and familiarity using the NovaSure
system;
• review and be familiar with the instructions and complete either
NovaSure training or be trained by a qualified physician;
• be aware of the appropriate sequence of actions detailed in the
Instructions for Use and Troubleshooting sections of this manual to
abort, resolve and/or continue the treatment in the event the system
detects a loss of CO2 during the cavity integrity assessment (CIA),
which indicates a possible uterine perforation.
Adjunct personnel must be familiar with these instructions and other
training materials prior to using the NovaSure system.
System Description
The NovaSure impedance controlled endometrial ablation system
consists of the NovaSure disposable device with connecting cord,
NovaSure RF controller (controller), NovaSure CO2 canister, desiccant,
foot switch and power cord, which are designed to be used together as
a system.
NovaSure Disposable Device with Connecting Cord,
Including Suction Line Desiccant
NovaSure®
Instructions for Use and Controller
Operator’s Manual
Table of Contents
Physician Checklist ..................................1
System Description ..................................1
Indications .........................................3
Patient Target Group .................................3
Intended Clinical Benefits to Patients ....................3
Intended User .......................................3
Contraindications ...................................3
Warnings ..........................................4
Precautions ........................................5
NovaSure 3-Year Clinical Data .........................6
Adverse Events ....................................6
Anticipated Post-Procedural Complications ...............6
Other Adverse Events ...............................6
Clinical Study .....................................7
Patient Selection ................................... 9
Patient Counseling ................................10
Pretreatment Preparation of Patient .................... 10
NovaSure Impedance Controlled Endometrial Ablation System
Instructions For Use ................................10
Operating the Model 10 RF Controller ..................15
Periodic Maintenance and Service ....................16
NovaSure Model 10 RF Controller Screen Icons ...........17
Troubleshooting Most Common Alarms .................17
Replacement Instructions ............................19
Technical Specifications .............................19
NovaSure disposable device .........................19
NovaSure RF controller .............................20
Environmental Conditions ..........................20
Important Performance Characteristics ................21
Electromagnetic Safety Guidance .....................21
Cleaning and Sanitizing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Parts List .......................................23
Disposal ..........................................23
Warranty .........................................23
Technical Support and Product Return Information. . . . . . . . 24
Symbol Glossary ...................................25

2
ENGLISH
NovaSure Disposable Device Description
The NovaSure disposable device consists of a single-patient use,
conformable bipolar electrode array mounted on an expandable frame
that can create a confluent lesion on the entire interior surface area
of the uterine cavity. The disposable device is inserted transcervically
into the uterine cavity, and the sheath is retracted to allow the bipolar
electrode array to be deployed and conform to the uterine cavity.
The bipolar electrode array is formed from a metalized, porous fabric
through which steam and moisture are continuously suctioned from
the desiccated tissue. The disposable device works in conjunction
with a dedicated NovaSure RF controller to perform customized, global
endometrial ablation in an average of approximately 90seconds without
the need for concomitant hysteroscopic visualization or endometrial
pretreatment. The specific configuration of the bipolar electrode array
and the predetermined power of the controller create a controlled depth
of ablation in uteri sounding less than or equal to 10cm and having a
minimum cornu-to-cornu distance of 2.5cm.
During the ablation process, the flow of radio frequency (RF) energy
vaporizes and/or coagulates the endometrium regardless of its thickness
and desiccates and coagulates the underlying, superficial myometrium.
The controller automatically calculates the optimal power level (W)
required for the treatment of the uterine cavity, based on uterine size.
As tissue destruction reaches an optimal depth, increasing tissue
impedance causes the controller to automatically terminate power
delivery, thereby providing a self-regulating process. Blood, saline and
other liquid present in the uterine cavity at the time of the procedure,
as well as vapor liberated from the desiccated tissue, are evacuated by
continuous, automatic suctioning.
The disposable device is connected to the controller via a cord
containing the RF cable, suction tubing used for pressure monitoring
during the cavity integrity assessment cycle and for suction during the
ablation cycle, and vacuum feedback tubing used for carbon dioxide
delivery during the cavity integrity assessment cycle and vacuum
monitoring during the ablation cycle. The disposable device has been
sterillized with ethylene oxide (EO).
NovaSure Model 10
RF Controller
NovaSure RF Controller Description
The NovaSure RF controller is a constant power output generator with a
nominal maximum power delivery capability of 180 watts. The controller
automatically calculates the power output based on the uterine cavity
length (sound measurement minus the length of the endocervical canal)
and width measurements that the user key-enters into the controller.
Monitoring tissue impedance during the ablation process automatically
controls the depth of endo-myometrial ablation. The NovaSure procedure
self-terminates once endometrial vaporization and superficial myometrial
desiccation have reached approximately 50ohms of impedance at the
tissue-electrode interface, or when the treatment timer reaches two
minutes. Integral to the controller is the cavity integrity assessment
system (CIA) which is designed to determine whether there is a defect
or perforation in the wall of the uterus. After the disposable device is
placed into the uterine cavity, CO2 is delivered through the central lumen
of the disposable device into the cavity, via the vacuum feedback tubing,
at a safe flow rate and pressure. If the CO2 pressure in the cavity is
maintained for a short period of time, indicating that the uterine cavity is
intact, then the CIA will allow the NovaSure RF controller to be enabled
and proceed with the treatment phase. A vacuum pump contained
within the NovaSure RF controller creates and maintains a vacuum in
the uterine cavity throughout the endometrial ablation procedure. Once
the vacuum is stabilized, the vacuum level is monitored throughout the
remainder of the ablation process.

3
ENGLISH
NovaSure Suction Line Desiccant
Description
The NovaSure suction line desiccant
is a non-sterile, single-patient use
component that the user attaches
in-line with the suction tubing, prior
to connecting the disposable device
to the NovaSure RF controller. The
desiccant absorbs the moisture
removed from the uterine cavity via
the suction tubing during the ablation
procedure.
NovaSure Foot Switch Description
The NovaSure foot switch is a
pneumatic switch that connects to the
NovaSureRFcontroller front panel. It
is used to activate the NovaSure RF
controller and does not contain any
electrical components.
NovaSure CO2 Canister
Description
The NovaSure CO2 canister is a 16-
gram CO2 (USP) canister. It is attached
to the regulator located on the back
panel of the NovaSureRFcontroller
prior to applying line voltage to
the NovaSureRFcontroller. The
CO2 is used by the cavity integrity
assessment system to pressurize the
uterine cavity.
The CO2 canister PN: 815012 is at
least 99% CO2.
NovaSure AC Power Cord
Description
The NovaSure AC power cord,
a medical grade cord, connects
the NovaSure RF controller to
the appropriate line voltage. The
receptacle for the power cord, the
power input module, is located on
the back panel of the NovaSure RF
controller.
Indications
The NovaSure system is intended to ablate the endometrial lining of the
uterus in pre-menopausal women with menorrhagia (excessive bleeding)
due to benign causes for whom childbearing is complete.
Patient Target Group
The NovaSure system is intended for use on pre-menopausal women
with menorrhagia (excessive bleeding) due to benign causes for whom
childbearing is complete.
Intended Clinical Benefits to Patients
To reduce or eliminate bleeding in pre-menopausal women with Heavy
Menstrual Bleeding due to benign causes for whom childbearing is
complete.
Intended User
The NovaSure System will be used under control and guidance of an OB/
GYN physician or GYN physician or surgeon. The physician will primarily
operate the NovaSure device and may provide instructions to the
assistant on the operation of the RF Controller and activate the controller
using the foot switch. The RF Controller will be operated by a non-sterile
assistant.
The physician must:
• Have sufficient experience in performing procedures within the uterine
cavity, such as IUD insertion or dilation and curettage (D&C) and with
adequate training, knowledge and familiarity using the NovaSure
system.
• Review and be familiar with the instructions and complete either
NovaSure training or be trained by a qualified physician.
Adjunct personnel must be familiar with the Instructions for Use and
other training materials prior to using the NovaSure system.
Contraindications
The NovaSure impedance controlled endometrial ablation system is
contraindicated for use in:
• a patient who is pregnant or who wants to become pregnant in the
future. Pregnancies following ablation can be dangerous for both
mother and fetus.
• a patient with known or suspected endometrial carcinoma (uterine
cancer) or pre-malignant conditions of the endometrium, such as
unresolved adenomatous hyperplasia.
• a patient with any anatomic condition (e.g., history of previous
classical cesarean section or transmural myomectomy) or pathologic
condition (e.g., long-term medical therapy) that could lead to
weakening of the myometrium.
• a patient with active genital or urinary tract infection at the time of
the procedure (e.g., cervicitis, vaginitis, endometritis, salpingitis or
cystitis).
• a patient with an intrauterine device (IUD) currently in place.
Presence of an IUD in the uterine cavity can interfere with a NovaSure
procedure.
• a patient with a uterine cavity length less than 4cm. The minimum
length of the electrode array is 4cm. Treatment of a uterine cavity with
a length less than 4cm will result in thermal injury to the endocervical
canal.
• a patient with a uterine cavity width less than 2.5cm, as determined
by the WIDTH dial of the disposable device following device
deployment.
• a patient with active pelvic inflammatory disease.

4
ENGLISH
Warnings
FAILURE TO FOLLOW ANY INSTRUCTIONS OR FAILURE TO HEED
ANY WARNINGS OR CAUTIONS COULD RESULT IN SERIOUS PATIENT
INJURY.
THE NOVASURE DISPOSABLE DEVICE MUST BE USED ONLY IN
CONJUNCTION WITH THE NOVASURE RF CONTROLLER.
THE NOVASURE PROCEDURE IS INTENDED TO BE PERFORMED ONLY
ONCE DURING A SINGLE OPERATIVE VISIT. THERMAL INJURY TO THE
BOWEL MAY OCCUR WHEN MULTIPLE NOVASURE THERAPY CYCLES
ARE PERFORMED DURING THE SAME OPERATIVE VISIT.
Uterine Perforation
• Use caution not to perforate the uterine wall when sounding, dilating
or inserting the disposable device.
• If the disposable device is difficult to insert into the cervical canal,
use clinical judgment to determine whether or not further dilation is
required.
• The NovaSure system performs a cavity integrity assessment (CIA)
to evaluate the integrity of the uterine cavity and sounds an alarm
warning of a possible perforation prior to treatment (Step 2.36).
(Although designed to detect a perforation of the uterine wall, it is
an indicator only and it might not detect all perforations under all
possible circumstances. Clinical judgment must always be used.)
• If a uterine perforation is suspected, the procedure should be
terminated immediately.
• If the cavity integrity assessment fails after reasonable attempts
to implement the troubleshooting procedures (step 2.36), abort
the procedure.
• For patients in whom the procedure was aborted due to a suspected
uterine wall perforation, a work-up for perforation should be
considered prior to discharge.
General
• Endometrial ablation using the NovaSure system is not a sterilization
procedure. Therefore, the patient should be advised of appropriate
birth control methods.
• Endometrial ablation does not eliminate the potential for endometrial
hyperplasia or adenocarcinoma of the endometrium and may mask the
physician’s ability to detect or make a diagnosis of such pathology.
• Endometrial ablation is intended for use only in women who do
not desire to bear children because the likelihood of pregnancy is
significantly decreased following the procedure. Pregnancy following
ablation may be dangerous for both mother and fetus.
• Patients who undergo endometrial ablation procedures who have
previously undergone tubal ligation are at increased risk of developing
post ablation tubal sterilization syndrome which can require
hysterectomy. This can occur as late as 10years post procedure.
• A health hazard may exist in the case where the NovaSure procedures
is performed in the presence of a thermally and electrically conductive
metal micro-insert that is improperly positioned (e.g., perforating the
fallopian tube or the myometrium). If this occurs, heat can be drawn
away from the intended treatment area toward other tissue and/or
organs in contact with the conductive object, which may be sufficient
to cause localized burns. As a result, correct placement of the metal
micro-insert must be confirmed prior to performing the NovaSure
procedure.
Technical
• Do not use the sterile, single-patient use disposable device if the
packaging appears to be damaged or there is evidence of tampering.
• The disposable device is for single-patient use only. Do not reuse or
re-sterilize the disposable device. The risk of reusing the disposable
device includes but is not limited to the following:
• ineffective procedure
• infection (major)
• electric shock
• transmission of communicable disease
• cervical laceration
• uterine perforation
• If any hysteroscopy procedure is performed with hypotonic solution
immediately prior to NovaSure treatment, then the uterine cavity must
be flushed with normal saline prior to treatment with the NovaSure
system. The presence of hypotonic fluid may reduce the efficiency of
the NovaSure system.
• Plugging the disposable device into the controller starts CO2 flow to
purge any air out of the disposable device and tubing. This purging
operation takes approximately 10seconds and must be performed
with the disposable device external to the patient to eliminate
the risk of air or gas embolism. A purging device screen appears on
the Model 10 RFC and an audible pulsed tone sounds throughout the
purge procedure. When the tone and the LED/screen message stops it
is safe to insert the disposable device.
• For patients with cardiac pacemakers or other active implants, a
possible hazard exists due to interference with the action of the
pacemaker that may occur and may damage the pacemaker. Consult
the pacemaker manufacturer for further information when use of the
NovaSure system is planned in patients with cardiac pacemakers.
• Care should be taken to ensure the patient does not contact metal
parts which are earthed or which have an appreciable capacitance to
earth.
• Danger: explosion hazard. Do not use in the presence of a flammable
anesthetic mixture. Do not use in the presence of flammable gases or
liquids.
• Failure of the NovaSureRFcontroller could result in an unintended
increase in output power.
Precautions
• It has been reported in the literature that patients with a severely
anteverted, retroflexed or laterally displaced uterus are at greater risk
of uterine wall perforation during any intrauterine manipulation.

5
ENGLISH
• A false passage can occur during any procedure in which the uterus
is instrumented, especially in cases of severe anteverted retroflexed
or a laterally displaced uterus. Use caution to ensure that the device is
properly positioned in the uterine cavity.
• The NovaSure system consists of the following components:
- single-patient use NovaSure disposable device with connecting cord
- NovaSure RF controller
- NovaSure CO2 canister
- NovaSure desiccant
- NovaSure foot switch
- power cord
To ensure proper operation, never use other components with the
NovaSure system. Inspect the components regularly for damage,
and do not use them if damage is apparent. The use of any cables or
accessories other than those specified in these instructions may result
in increased emissions or decreased immunity of the RF controller.
• The RF controller must be installed and put into service according
to the guidance provided in these instructions to ensure its
electromagnetic compatibility. Refer to the electromagnetic emissions
and immunity tables in the Specifications section.
• The RF controller should not be used adjacent to or stacked with other
equipment. If adjacent or stacked use is necessary, the RF controller
should be observed to verify normal operation in the configuration in
which it will be used.
• Portable and mobile RF communications equipment can affect the
RF controller. Refer to the electromagnetic immunity tables in the
Specifications section for recommended separation distances.
• Patients who have undergone endometrial ablation and are later
placed on hormone replacement therapy should have a progestin
included in their medication regimen in order to avoid the increased
risk of endometrial adenocarcinoma associated with unopposed
estrogen replacement therapy.
• The safety and effectiveness of the NovaSure system has not been
fully evaluated in patients:
- with a uterine sound measurement greater than 10cm;
- with submucosal fibroids that distort the uterine cavity;
- with bicornuate, septate or sub-septateuteri;
- with medical (e.g., GnRH agonist) or surgical pretreatment;
- who have undergone a previous endometrial ablation including the
NovaSure endometrial ablation procedure; or,
- who are post-menopausal.
• Do not attempt to repair the controller if problems are suspected.
Call Hologic Technical Support or a Hologic sales representative for
instructions.
• Cables to the disposable device should be positioned such that contact
with patient or other leads is avoided.
• The user should inspect the disposable device for damage prior to use.
• The suction line desiccant is non-sterile, and the packaging should not
be placed in the sterile field.
• If an Array Position message is displayed on the Model 10 screen,
see the Troubleshooting section under “ARRAY POSITION ALARM”
• Do not use the NovaSure suction line desiccant if desiccant material is
pink in color.
• The disposable device must be external to (outside of) the patient
before connecting the cord to the appropriate port on the front panel of
the controller (step 2.15).
• The carbon dioxide canister contains gas under high pressure. In the
event of a breached CO2 canister or line, allow the canister to exhaust
completely, and allow the canister and/or lines to equilibrate to room
temperature prior to handling.
• CO2 continuously flows from the time that the disposable device is
plugged into the controller until the CIA portion of the procedure is
complete. To minimize the duration of CO2 flow and potential risk of
embolism, perform the seating procedure immediately after inserting
the disposable device and proceed directly from the seating procedure
to the CIA.
• Electrically conductive objects (e.g., monitoring electrodes from other
devices) that are in direct contact with the electrode array of the
disposable device or in close proximity to the electrode array may
draw current away from the array. This may result in localized burns
to the patient or physician or in distortion of the electrical field of the
array, which would change the therapeutic effect (under-treatment or
over-treatment). It may also result in distortion of the current in the
conductive object, e.g., monitors may display false readings.
• Grounding reliability is only achieved when equipment is connected to
a receptacle marked “hospital grade”.
• To avoid risk to patient and operators, do not use this equipment in
the presence of intentional magnetic sources, intentional ultrasound
sources, or intentional heat sources.
• The cervical collar must be fully retracted to its proximal position in
order to minimize the potential for damage to the sheath when closing
the array.
• The NovaSure device is contraindicated for use in pregnant women
or women that want to become pregnant in the future. Pregnancies
following ablation can be dangerous for both mother and fetus. Sound
medical judgment should be used.

6
ENGLISH
NovaSure 3-Year Clinical Data
Adverse Events
The NovaSure system was evaluated in a randomized, prospective,
multi-center clinical study of 265patients with abnormal uterine
bleeding comparing the NovaSure system to a control arm of wire loop
resection of the endometrium followed by rollerball ablation.
Table 1A. Intra-Operative Adverse Events
Adverse Event
NovaSure
n=175 (%)
Loop Resection
Plus Rollerball
n=90 (%)
Bradycardia 1 (0.6%) 0 (0.0%)
Uterine perforation 0 (0.0% 3 (3.3%)
Cervical tear 0 (0.0% 2 (2.2%)
Cervical stenosis 0 (0.0% 1 (1.1%)
TOTAL 1 (0.6%) 6 (6.7%)
Table 1B. Post-Operative Adverse Events < 24 Hours
Adverse Event
NovaSure
n=175 (%)
Loop Resection
Plus Rollerball
n=90 (%)
Pelvic pain/cramping 6 (3.4%) 4 (4.4%)
Nausea and/or vomiting 3 (1.7%) 1 (1.1%)
TOTAL 9 (5.1%)* 5 (5.6%)**
* Nine events reported in 6 (3.4%) patients
** Five events reported in 4 (4.4%) patients
Table 1C. Post-Operative Adverse Events > 24 Hours – 2 Weeks
Adverse Event
NovaSure
n=175 (%)
Loop Resection
Plus Rollerball
n=90 (%)
Hematometra 1 (0.6%) 0 (0.0%
Urinary tract infection 1 (0.6%) 1 (1.1%)
Vaginal infection 1 (0.6%) 0 (0.0%
Endometritis 0 (0.0% 2 (2.2%)
Pelvic inflammatory disease 0 (0.0% 1 (1.1%)
Hemorrhage 0 (0.0% 1 (1.1%)
Pelvic pain/cramping 1 (0.6%) 1 (1.1%)
Nausea and/or vomiting 1 (0.6%) 1 (1.1%)
TOTAL 5 (2.9%)* 7 (7.8%)**
* Five events reported in 4 (2.3%) patients
** Seven events reported in 6 (6.7%) patients
Table 1D. Post-Operative Adverse Events > 2 Weeks – 1 Year
Adverse Event
NovaSure
n=175(%)
Loop Resection
Plus Rollerball
n=90 (%)
Hysterectomy 3 (1.7%) 2 (2.2%)
Hematometra 1 (0.6%) 2 (2.2%)
Urinary tract infection 2 (1.1%) 2 (2.2%)
Vaginal infection 5 (2.9%) 2 (2.2%)
Endometritis 2 (1.1%) 1 (1.1%)
Pelvic inflammatory disease 2 (1.1%) 0 (0.0%
Hemorrhage 1 (0.6%) 0 (0.0%
Pelvic pain/cramping 5 (2.9%) 6 (6.7%)
TOTAL 21 (12.0%)* 15 (16.17%)**
* 21 events in 19 (10.9%) patients
** 15 events in 15 (16.7%) patients
Anticipated Post-Procedural Complications
For any endometrial ablation procedure, commonly reported post-
operative events include the following:
• Cramping/pelvic pain was reported for 3.4% of the NovaSure patients
and 4.4% of the wire resection loop plus rollerball-treated patients
within 24hours of the procedure. Postoperative cramping can range
from mild to severe. This cramping will typically last a few hours and
rarely continues beyond the first day following the procedure.
• Nausea and vomiting were reported for 1.7% of the NovaSure patients
and 1.1% of the wire loop resection plus rollerball patients within
24hours of the procedure. When present, nausea and vomiting
typically occur immediately following the procedure, are associated
with anesthesia and can be managed with medication.
• Vaginal discharge
• Vaginal bleeding/spotting
Other Adverse Events
As with all endometrial ablation procedures, serious injury or death can occur.
The following adverse events could occur or have been reported in
association with the use of the NovaSure system:
• post-ablation tubal sterilization syndrome
• pregnancy-related complications (NOTE: PREGNANCY FOLLOWING
ENDOMETRIAL ABLATION IS VERY DANGEROUS FOR BOTH THE
MOTHER AND THE FETUS.)
• thermal injury to adjacent tissue
• perforation of the uterine wall
• difficulty with defecation or micturition
• uterine necrosis
• air or gas embolism
• infection or sepsis
• complications leading to serious injury or death

7
ENGLISH
Clinical Study
Purpose: Safety and effectiveness of the use of the NovaSure system
was compared to wire loop resection of the endometrium followed by
rollerball ablation in premenopausal women suffering from menorrhagia
secondary to benign causes.
Pretreatment: Patients randomized into the NovaSure arm received
no endometrial pretreatment (e.g., hormone, D&C or patient timing).
Patients randomized into the control arm received wire loop resection as
an endometrial pretreatment.
Study endpoints: The primary effectiveness measure was a validated
menstrual diary scoring system developed by Higham (Higham JM,
O’Brien PMS, Shaw RW Br J Obstet Gynaecol 1990; 97:734-9).
Assessment of menstrual blood loss was performed using a pictorial
blood loss assessment chart (PBLAC). Patient success was defined as
a reduction in menstrual flow at 1 year post-procedure to a diary score
of <75. Study success was defined as a statistical difference of less
than 20% in patient success rates between the NovaSure impedance
controlled endometrial ablation system and wire loop resection plus
rollerball ablation. Patients were contacted at two and three years and
asked a series of questions regarding their bleeding over the previous
12months. Each patient’s menstrual bleeding status was determined
at two and three years using the one-year PBLAC score and bleeding
pattern as a reference. Thus, it was possible to directly compare a
patient’s bleeding pattern or menstrual status at one year to the bleeding
pattern at two and three years.
Secondary endpoints included anesthesia regimen, length of procedure
and responses from a quality-of-life questionnaire. Safety evaluation was
based on the adverse events reported during the study.
Methods: A randomized (2:1), prospective clinical study was conducted
at 9clinical sites and included 265patients diagnosed with menorrhagia.
Menstrual diary scores were collected pre-operatively and monthly for
12months post-procedure. Patients were treated at any time in their
menstrual cycle. None of the patients received hormonal pretreatment
to thin the endometrial lining. Control patients received hysteroscopic
wire loop resection of the endometrium as a mechanical means of
endometrial pretreatment followed by rollerball ablation. Study subjects
were required to meet the following key patient selection criteria:
Inclusion criteria
• Refractory menorrhagia with no definable organic cause (dysfunctional
uterine bleeding)
• Ages 25 to 50years of age
• Uterine sound measurement of 6.0–10.0cm (external os to internal
fundus)
• Minimum PBLAC score of >150 for 3months prior to study enrollment;
or PBLAC score >150 for one month for women who:
- had at least 3 prior months (documented) failed medical therapy;
- had a contraindication to medical therapy; or
- refused medical therapy.
Exclusion criteria
• Presence of bacteremia, sepsis or other active systemic infection
• Active or recurrent chronic pelvic inflammatory disease
• Patient with documented coagulopathies or on anticoagulants
• Symptomatic endometriosis
• Prior uterine surgery (except low segment cesarean section)
that interrupts the integrity of the uterine wall e.g., transmural
myomectomy or classical cesarean section
• Prior endometrial ablation
• Patient on medications that could thin the myometrial muscle, such as
long-term steroid use
• Patient desire to have children or to preserve fertility
• Patient currently on hormonal birth control therapy or unwilling to use
a non-hormonal birth control post-ablation
• Abnormal/obstructed cavity as confirmed by hysteroscopy, SIS or HSG.
Specifically:
- septate or bicornuate uterus or other congenital malformation of the
uterine cavity
- pedunculated, submucous leiomyomata or other leiomyomata which
distort the cavity; polyps (larger than 2cm) which are likely to be the
cause of the patient’s menorrhagia
- presence of an IUD
• Suspected or confirmed uterine malignancy within the last five years
as confirmed by histology
• Endometrial hyperplasia as confirmed by histology
• Unaddressed cervical dysplasia
• Elevated FSH levels consistent with ovarian failure >40IU/ml
• Pregnancy
• Active sexually transmitted disease
Patient population: A total of 265patients were enrolled in this study.
Patients were between the ages of 25 to 50 with 46% under the age
of 40 and 54% 40years of age or older. There were no differences in
demographic or gynecological history parameters between the treatment
groups, between the age groupings or among the nine investigational sites.
Table 2. Patient Accountability
Number of Patients NovaSure Wire Loop
Resection
Plus Rollerball
Entered into Study
(Intent-to-Treat population) 175 90
Aborted procedures*1-4 -2
Treated 171 88
Additional treatment* -4 -2
Hysterectomy*2-3 -2
Lost to follow-up* -5 -2

8
ENGLISH
Table 2. Patient Accountability
Number of Patients NovaSure Wire Loop
Resection
Plus Rollerball
Hodgkin’s disease* -1 0
Pelvic Pain - administered
leuprolide*
-1 0
12-Month
follow-up data available 157 82
Additional treatment* -2 -1
Hysterectomy*2-3 -1
Lost to follow-up* -2 -5
Missed visit -1 -1
Declined to participate* -1 0
Pregnancy* -1 0
24-Month
follow-up data available 147 74
Additional treatment* 0 -4
Hysterectomy*2-5 -1
Lost to follow-up* -4 -2
36-Month follow-up 138 67
Subject lost to follow-up at
24 mos., returned at 36 mos.
+1 +1
36-Month follow-up data
available 139 68
* Discontinued patients
1 Four NovaSure did not meet protocol Inclusion Criteria; Two Rollerball had uterine perforation
2 For hysterectomy, see Table 7
Results
Primary effectiveness endpoint: bleeding score
Patient success at 12-months post-procedure is defined as a reduction
in diary score from >150 pre-operatively to <75 post-procedure.
Amenorrhea is defined as a score of 0. Success at 24 and 36 months,
based on telephone questionnaires, is defined as elimination of bleeding
or reduction to light or normal flow. Data presented in Table 3 (below)
represent the clinical results based on the total number of 265 patients
randomized (Intent-to-Treat group (ITT)) for the study. The worst-case
scenario is presented whereby each of the discontinued patients
(described in Table 2 for patient accountability) is counted as a “failure”
for calculating the values listed in the table.
Table 3. Effectiveness: Success Rates–Intent-To-Treat Patients
NovaSure
(n=175)
Wire Loop Resection
Plus Rollerball
(n=90)
Months post ablation 12* 24** 36** 12* 24** 36**
Table 3. Effectiveness: Success Rates–Intent-To-Treat Patients
NovaSure
(n=175)
Wire Loop Resection
Plus Rollerball
(n=90)
Number of
successful patients 136 143 134 67 68 63
Study success rate 77.7% 81.7% 76.6% 74.4% 75.6% 70.0%
# of patients with
Amenorrhea 63 64 58 29 26 23
Amenorrhea rate 36.0% 36.6% 33.1% 32.2% 28.9% 25.6%
* Based on diary scores
** Based on telephone questionnaires
Secondary effectiveness endpoint: quality of life
Patient quality of life (QOL) was assessed by administering the quality of
life questionnaire (SF-12) and the menstrual impact questionnaire prior
to treatment and at 3, 6, 12, 24 and 36months post-procedure. Table4
shows the patient responses for both groups pre-operatively, where
appropriate, and at 12, 24 and 36months post-procedure.
Table 4. Effectiveness: Quality of Life (QOL)
NovaSure Wire Loop Resection Plus
Rollerball
Number of Patients Responding to Quality of Life Questionaire#
Pre-operatively 175 90
12 Months 154 82
24 Months 143 73
36 Months 139 67
Percent of Patients Satisified Or Very Satisified
12 Months 92.8% 93.9%
24 Months 93.9% 89.1%
36 Months 96.3% 89.7%
Percent of Patients Who Probably Or Definitely Would Recommend This
Procedure
12 Months 96.7% 95.9%
24 Months 96.6% 94.5%
36 Months 97.8% 92.6%
Percent of Patients with Dysemenorrhea
Pre-operatively 57.1% 55.6%
12 Months 20.8%& 34.2%*,&
24 Months 20.3%* 30.1%*
36 Months 17.3%* 28.4%*
Percent of Patients with PMS
Pre-operatively 65.1% 66.7%
12 Months 36.4%* 35.4%*
24 Months 44.0%* 46.6%*
36 Months 34.5%* 41.2%*
Percent of Patients Reporting Sometimes, Frequently Or Always Have
Difficulty Performing Work Or Other Activities Due to Menses
Pre-operatively 66.3% 65.5%

9
ENGLISH
Table 4. Effectiveness: Quality of Life (QOL)
NovaSure Wire Loop Resection Plus
Rollerball
12 Months 9.9%* 8.6%*
24 Months 14.5%* 15.0%*
36 Months 16.3%* 13.3%*
Percent of Patients Reporting Sometimes, Frequently Or Always Feel
Anxious Due to Menses
Pre-operatively 74.7% 68.9%
12 Months 23.6%* 18.5%*
24 Months 24.2%* 19.2%*
36 Months 18.7%* 19.1%*
Percent of Patients Reporting Sometimes, Frequently Or Always Miss
Social Activities Due to Menses
Pre-operatively 63.3% 62.2%
12 Months 8.5%* 8.6%*
24 Months 9.0%* 11.1%*
36 Months 8.1%* 10.8%*
# Not all patients completed questionnaire
* Statistically significant difference from pre-operative response (Chi-Square; p<0.05)
& Statistically significant difference between NovaSure and Rollerball Groups
(Chi-Square; p=0.02)
Safety endpoint
Adverse event information is described in the “Adverse Events” section of this manual.
Secondary endpoint: procedure time
Procedure time, a secondary endpoint, was determined for each patient
by recording the time of device insertion and the time of device removal.
The mean procedure time for the NovaSure patients was significantly
less than the procedure time for the rollerball group, (4.2 ±3.5 minutes
and 24.2 ±11.4 minutes, respectively). Mean time for application of RF
energy was 84.0 ±25.0 seconds in a subset of monitored NovaSure
patients (Table5).
Table 5. Operative Procedure Time
Operative Parameters NovaSure
n=175
Wire Loop Resection
Plus Rollerball
n=90
Number of treated patients* 171 88
Procedure time minutes (± SD)
(Device insertion to device
removal)
4.2 ± 3.5** 24.2 ± 11.4**
Procedure time in seconds (±SD)
(Time of energy delivery)
84.0 ± 25.0 ND#
* See Table 2 for patient accountability
** Statistically significant difference between treatment groups (Student’s t-test; p < 0.05)
# Not determined
Secondary endpoint: anesthesia regimen
Anesthesia was left to the discretion of each patient, clinical investigator
and attending anesthesiologist. For the NovaSure patients, 27.0%
(47/174) had the procedure performed under general anesthesia or
epidural and 73.0% (127/174) under local and/or IV sedation. One
patient did not have a reported anesthesia regimen in this group. In
the rollerball group, 82.2% (74/90) of the patients were treated under
general anesthesia or epidural and 17.8% (16/90) under local and/or IV
sedation (Table6).
Table 6. Anesthesia Regimen
NovaSure
n=175*
Wire Loop Resection
Plus Rollerball
n=90
General or epidural 27.0% 82.2%
Local and/or IV sedation 73.0% 17.8%
* One patient did not have a reported anesthesia regimen.
Clinical observations
Hysterectomy
Fifteen women had a hysterectomy within the three years following the
ablation procedure. Table7 lists the reasons for hysterectomy.
Table 7. Hysterectomy
Reason For Hysterectomy NovaSure
n=175
Wire Loop Resection
Plus Rollerball
n=90
Adenocarcinoma diagnosed at
time of ablation procedure 1 1
Fibroids 2 0
Pelvic abscess 1 1
Endometriosis 3 0
Adenomyosis 4 0
Hematometra 0 1
Menorrhagia 0 1
TOTAL 11 (6.3%) 4 (4.4%)
7Hysterectomies were in patients <40years (7 NovaSure) and 8hysterectomies were in patients >40years
(4NovaSure; 4 Rollerball).
Patient Selection
Menorrhagia can be caused by a variety of underlying problems,
including, but not limited to; endometrial cancer, myomas, polyps, drugs
and dysfunctional uterine bleeding (anovulatory bleeding). Patients
always should be screened and evaluated to determine the cause of
excessive uterine bleeding before any treatment option is initiated.
Consult medical literature relative to various endometrial ablation
techniques, indications, contraindications, complications and hazards
prior to the performance of any endometrial ablation procedure.
Patient Counseling
As with any procedure, the physician needs to discuss risks, benefits
and alternatives with the patient prior to performing endometrial
ablation. Patient’s expectations should be set in a way that the patient
understands that the aim of the treatment is the reduction in bleeding to
normal levels.

10
ENGLISH
The disposable device is intended for use only in women who do
not desire to bear children because the likelihood of pregnancy is
significantly decreased following the procedure. Patients of childbearing
capacity should be cautioned of potential complications, which may
ensue if they should become pregnant. This counseling should include
the need for post-procedure contraception where indicated. This
procedure is not a sterilization procedure and subsequent pregnancies
may be dangerous for the mother and fetus.
Vaginal discharge is typically experienced during the first few weeks
following ablation and may last as long as a month. Generally,
the discharge is described as bloody during the first few days;
serosanguineous by approximately one week; then profuse and watery
thereafter. Any unusual or foul-smelling discharge should be reported to
the physician immediately. Other common post-procedural complications
include cramping/pelvic pain, nausea and vomiting.
Uterine perforation should be considered in the differential diagnosis of
any post-operative patient complaining of acute abdominal pain, fever,
shortness of breath, dizziness, hypotension or any other symptom that
may be associated with uterine perforation with or without damage
to the adjacent organs of the abdominal cavity. Patients should be
counseled that any such symptoms should be immediately reported to
their physician.
Pretreatment Preparation of Patient
The NovaSure impedance controlled endometrial ablation system
successfully treats a uterine cavity over a range of endometrium
thickness. The lining of the uterus does not have to be thinned prior to
the procedure, and the procedure may be performed during either the
proliferative or the secretory phase of the cycle. Although the safety and
effectiveness of the NovaSure system has not been fully-evaluated in
patients with medical or surgical pretreatment, it has been evaluated in a
limited number of patients who had been pretreated with GnRH agonists
with no complications or adverse events.
Active bleeding was not found to be a limiting factor when using
the NovaSure system. It is recommended that a nonsteroidal anti-
inflammatory drug (NSAID) be given at least one hour prior to treatment
and continued postoperatively to reduce intraoperative and postoperative
uterine cramping.
NovaSure Impedance Controlled Endometrial Ablation
System Instructions For Use
Please read all instructions, cautions and warnings prior to use.
1.0 Set-up
NOVASURE
RF CONTROLLER
NOVASURE DISPOSABLE DEVICE
WITH CONNECTING CORD,
INCLUDING SUCTION LINE
DESICCANT
NOVASURE POWER CORD NOVASURE SUCTION LINE
DESICCANT
NOVASURE CO2 CANISTER NOVASURE FOOT SWITCH
1.1 The following items are required when using the NovaSure system:
• one sterile, single-patient use NovaSure disposable device with
connecting cord
• one NovaSure RF controller
• one NovaSure foot switch
• one NovaSure AC power cord
• one NovaSure non-sterile suction line desiccant assembly
• one NovaSure CO2 canister.
Vacuum
Relief Valve
Cervical Collar
Bipolar
Electrode
Array
Front Handle
Sheath
Rear
Handle
Suction
Line
Lock Release
Button
Cavity Length Setting
Vacuum
Feedback
Line Barb
WIDTH Dial

11
ENGLISH
NOTE: Please have available at least one extra disposable device,
desiccant assembly and CO2 canister.
1.2 Prepare the NovaSure RF controller. Place it on a small table to one
side of the patient within visual field of the surgeon. Attach the AC
power cord to the controller and plug it into the AC outlet.
1.3 Screw the CO2 canister into the regulator on the back panel of the
controller until tightened.
Toggle
switch
CO2 canister
AC
power
cord
1.4 Fully rotate the CO2 regulator knob to the HI position (if equipped).
NOTE: Newer model controllers are not equipped with a knob on the
regulator, thus allowing the CO2 flow to be automatically regulated.
If your controller is not equipped with a regulator knob, proceed to
step1.5.
1.5 Press the toggle switch on the back panel of the controller into the
“on” position.
1.6 Connect the foot switch to the appropriate port on the front panel of
the controller.
NOTE: The first time the Model 10 RFC is turned on, the “Select Your
Language” screen will display. The default setting is in English. To
select another language, press the button with the name of that
language. Save the selection by pressing the flashing green button.
The language selection will be retained. To change the language
selection after the initial setup, use the “Settings” screen. Press the
name of the language to change the language used on the screen
display. To save changes to the settings, press the flashing green
button. To cancel a selection, press the Blue “X”.
2.0 Procedure
2.1 Prepare the patient for the anesthesia.
2.2 Place patient in dorsal lithotomy position.
2.3 Induce anesthesia according to standard practice.
2.4 Perform bimanual examination. Evaluate for severe anteversion or
retroversion.
Port
2.5 Prepare and drape patient similar to prep for D&C.
2.6 Insert a speculum into the vagina.
2.7 Grasp the cervix with a tenaculum.
2.8 Take a sound measurement of the uterus to measure the length
from fundus to external cervical os. The efficacy of the NovaSure
system has not been fully evaluated in patients with a uterine
sound measurement greater than 10cm.
2.9 Determine the length of the cervical canal and dilate the canal
for device insertion.
NOTE: The diameter of the NovaSure disposable device is a
nominal 6mm.
2.10 Using the uterine sound and cervical canal measurements, consult
the cavity length table (below) to obtain the appropriate cavity
length settings. On the upper end of the table, dimensions have
been adjusted to reflect the disposable device electrode length.
Correct determination of the cavity length is important for safe and
effective treatment. Overestimating the cavity length may result in
thermal injury to the endocervical canal.
WARNING: Use caution not to perforate the uterine wall when
sounding, dilating or inserting the disposable device.
TABLE 8. CAVITY LENGTH
Uterine Sound (cm)
Cervix
Length
(cm) 10 9.5 9 8.5 8 7.5 7 6.5 6
26.5* 6.5* 6.5* 6.5 6 5.5 5 4.5 4
2.5 6.5* 6.5* 6.5 6 5.5 5 4.5 4
36.5* 6.5 6 5.5 5 4.5 4
3.5 6.5 6 5.5 5 4.5 4
46 5.5 5 4.5 4
4.5 5.5 5 4.5 4
55 4.5 4
5.5 4.5 4
64
* The value of 6.5 is not intended to reflect the numerical difference between the sound length
and the length of the cervical canal.
The value 6.5 was entered because it represents the maximum length that the NovaSure
array can be extended.
CONTRAINDICATION: Do not treat a patient with a uterine cavity
length that is less than 4 cm, as cervical canal damage may occur.
NOTE: Patients with a uterine cavity length greater than 6.0cm had
observed success rates that were lower than overall study success
rates.
2.11 Open the sterile NovaSuredisposable device package. Place the
disposable device with the connecting cord into the sterile field

12
ENGLISH
while being careful to keep the non-sterile suction line desiccant
box out of the sterile field.
WARNING: Do not use the sterile single-patient use disposable device if
the packaging appears to be damaged or there is evidence of tampering.
2.12 Open the non-sterile suction line desiccant box and pouch.
Remove the red caps.
CAUTION: The suction line desiccant is non-sterile and the
packaging should not be placed in the sterile field.
CAUTION: If the suction line desiccant is pink, then replace it prior
to initiating the ablation procedure.
2.13 Connect the desiccant to the barbs on the suction tubing of
disposable device. Ensure the barbs are fully inserted into the
tubing on the desiccant.
2.14 CAUTION: Disposable device must be external to (outside of)
the patient before performing step 2.15.
2.15 Connect the disposable device cord to the appropriate port on the
front panel of the controller.
WARNING: Plugging the NovaSure disposable device into the
NovaSureRFcontroller starts CO2 flow to purge any air out of
the disposable device and tubing. The purging operation takes
approximately 10 seconds and must be performed with the
disposable device external to the patient. A purging device message
Disposable Device
Port
displays on the Model 10 RFC and an audible pulsed tone sounds
throughout the purge procedure. When the tone and the LED/screen
message stop, it is safe to insert the NovaSure disposable device.
CAUTION: CO2 continuously flows from the time that the disposable
device is plugged into the controller until the CIA portion of the
procedure is complete. To minimize the duration of CO2 flow
and potential risk of embolism, perform the seating procedure
immediately after inserting the disposable device and proceed
directly from the seating procedure to the CIA.
WARNING: Use caution not to perforate the uterine wall when
sounding, dilating or inserting the disposable device.
2.16 Deploy the disposable device outside of the patient and ensure
the screen message does not display on the Model 10 RFC when
the array is opened. If the screen message is still displayed on the
Model 10 RFC, close and open the disposable device again. If this
does not resolve the problem, replace the disposable device.
2.17 Be certain the WIDTH dial reads greater than or equal to 4.0cm.
WIDTH dial
NOTE: If the WIDTH dial reads less than 4.0cm, close the disposable
device and repeat step 2.16 above. If the WIDTH dial still reads
less than 4.0cm, open a new disposable device and return the old
disposable device to Hologic Technical Support.
2.18 Unlock the disposable device by pressing the lock release button.
Close the disposable device by holding the front handle stationary
and gently pulling the rear handle backwards until the closed array
indicator, located at the hinge of the front and rear handles, reads,
“ARRAY CLOSED”. This indicates that the array has been retracted
into the sheath and the disposable device is in the closed position.
ARRAY
CLOSED
indicator
Lock release
button
2.19 Make sure the array is completely enclosed by the external sheath.
2.20 Check that the WIDTH dial reads approximately 0.5cm.

13
ENGLISH
2.21 Using the uterine sound measurement and cervical canal
measurements, consult the cavity length table (above) to obtain the
appropriate cavity length settings as described in step 2.10 above.
CONTRAIDICATION: Do not treat a patient with a uterine cavity
length that is less than 4cm, as cervical canal damage may occur.
2.22 Using the cavity length table in section 2.10, select the value
obtained for length into the NovaSure RF controller input screen by
depressing the UP/DOWN arrows.
2.23 Adjust and lock the cavity length setting feature on the disposable
device to the value obtained above. (See step 2.21.) Ensure that the
cervical collar is fully retracted to its proximal position.
2.24 Confirm that the cervix is dilated to a minimum 6 mm (the nominal
diameter of the NovaSure disposable device).
2.25 Maintain a slight traction on the tenaculum to minimize the angle of
the uterus.
2.26 Angle the disposable device in-line with the axis of the uterus as
the disposable device is inserted transcervically into the uterine
cavity. By holding the front handle, advance the disposable device
until the distal end of the sheath touches the fundus.
#10
WARNING: If the disposable device is difficult to insert into the
cervical canal, use clinical judgment to determine whether or not
further dilation is required.
2.27 Withdraw the disposable device approximately 0.5 cm from the
fundus. Slowly squeeze the handles (DO NOT LOCK) up to the point
of increased resistance.
The WIDTH dial should read approximately 0.5 cm. At this point, the
external sheath has been retracted.
2.28 Continue to slowly squeeze the disposable device handles together
while gently moving the disposable device ~0.5 cm to and from
the fundus and rotating the handle of the disposable device 45°
counterclockwise from the vertical plane and 45° clockwise from
the vertical plane until the handles lock.
The WIDTH dial should read greater than 2.5 cm.
NOTE: Once the disposable device handles are locked, the uterus
should move in conjunction with the disposable device.
2.29 Gently move the disposable device using anterior, posterior and
lateral movements.
0.5 cm

14
ENGLISH
Gentle pressure
Slight pressure
2.33 Read the cornu-to-cornu measurement (2.5cm minimum) on the
WIDTH dial indicator.
CONTRAINDICATION: Do not treat a patient with a uterine cavity
width less than 2.5cm, as determined by the WIDTH dial of the
disposable device following device deployment.
CAUTION: If the ARRAY POSITION notification appears, see the
Troubleshooting section under “ARRAY POSITION Alarm.”
2.34 Select the value indicated on the WIDTH dial into the NovaSure RF
controller input screen by depressing the UP/DOWN arrows.
2.35 The system can be operated in either automatic mode or manual
mode. In automatic mode the ablation cycle will start automatically
upon successful completion of the cavity integrity assessment
(CIA). In manual mode the ablation cycle will not start automatically
following a successful CIA.
2.30 To complete placement, slightly pull back the disposable device
until the WIDTH dial reading reduces by approximately 0.2–0.5cm.
2.31 Hold the tenaculum, advance the disposable device slowly and
gently to the fundus. The WIDTH dial should read greater than or
equal to the previous measurement.
2.32 Slide the cervical collar forward using gentle pressure on the tab on
the cervical collar, until the cervical collar forms a seal against the
external cervical os.
NOTE: Correct placement of the electrode array against the fundus is important to safe and effective treatment. If part of the electrode array
or the distal edge of the external sheath is seated in the endocervical canal during treatment, there is an increased risk of endocervical
thermal injury.
Fundus
Electrode Array
Sheath Edge
Endocervical
Canal
Sheath edge resides in
lower uterine segment
Electrode Array
Endocervical
Canal
Sheath Edge
Sheath edge resides in
endocervical canal
Fundus
INCORRECT PLACEMENT CORRECT PLACEMENT

15
ENGLISH
Operating the Model 10 RF Controller
A. Automatic mode
To operate the Model 10 RFC in Automatic Mode, press the “Switch
Mode” button when it appears at the bottom of the screen. Proceed
to step 2.36, but do not follow step 2.37 if operating the system in
automatic mode.
B. Manual mode
NOTE: Manual Mode is the default system operation.
To operate the system in manual mode, do not press the “Switch Mode”
button prior to beginning the cavity integrity assessment (CIA).
Follow steps 2.36 and 2.37.
2.36 Begin the CIA procedure by stepping on the foot switch once.
“Cavity Assessment in Progress” will display on the screen while
five dots light off and on sequentially. The duration of the test
will range between approximately 7 and 30 seconds. A “Cavity
Assessment Complete” screen displays when the CIA has passed
and the system can deliver RF energy. Power cannot be applied to
the disposable device until the CIA Complete screen displays.
If the cavity integrity assessment fails, a screen will display “Cavity
Assessment Failure” with troubleshooting steps.
A. If a perforation is suspected, the procedure should be terminated
immediately.
B. If the CIA test fails again, check for leaks in the system, and
between the cervix and cervical collar. Be sure to check all tubing
connections, and ensure that a suction line desiccant has been
installed. If the leak appears to be at the cervix and cannot be
resolved by using the cervical collar, use another tenaculum to
grasp the cervix around the sheath. Repeat the CIA test by pressing
the foot switch.
NOTE: CO2 leakage may occur at the external cervical os due to the
presence of an over-dilated cervix. Visible bubbles or the “hissing”
sound of escaping gas may accompany CO2 leakage under either of
these conditions.
C. If the cavity integrity assessment fails after reasonable attempts to
implement the troubleshooting procedures (step 2.36), abort the
procedure.
NOTE: Removing the disposable device from the uterine cavity after
completing a cavity integrity assessment will require an additional
CIA test to be performed upon disposable device re-insertion
(whether or not the CIA previously passed) prior to initiating an
ablation.
2.37 Manual Mode Only
When operating the system in manual mode, the ablation cycle
will not start automatically after the successfully completion of the
cavity integrity assessment (CIA). Once a successful CIA has been
completed, press the ENABLE button and depress the foot switch a
second time to initiate the ablation cycle.
NOTE: In all Model 10 RF controllers, a vacuum pre-check occurs
automatically prior to initiation of the ablation cycle. A “Vacuum
Check in Progress” screen will appear and an audible tone will be
heard for up to 10 seconds during the vacuum pre-check.
During the ablation cycle, an “RF ON” screen with a timer will
appear to track the duration of the ablation.
NOTE: RF power delivery can be stopped at any time by pressing
the foot switch.
2.38 After automatic termination of the ablation cycle (approximately 90
seconds), fully retract the cervical collar to its proximal position by
using the tab on the cervical collar.
CAUTION: The cervical collar must be fully retracted to its proximal
position in order to minimize the potential for damage to the sheath
when closing the array.
Cervical
Collar

16
ENGLISH
At the completion of the ablation cycle, a “Procedure Complete” screen
will appear with a summary of the procedure. The “Procedure Complete”
screen will capture the following information for each procedure:
• Cavity Length
• Cavity Width
• Power Level
• RF Ablation Time
2.39 Unlock the disposable device by pressing the lock release button.
Close the disposable device by holding the front handle stationary
and gently pulling the rear handle backwards until the closed array
indicator, located at the hinge of the front and rear handles, reads
“ARRAY CLOSED”. This indicates that the array has been retracted
into the sheath and the disposable device is in the closed position.
NOTE: If it is difficult to close and remove the disposable device,
see the Troubleshooting section, “Difficulty closing and removing
the disposable device post-ablation”.
CAUTION: To avoid damaging the device, employ gentle technique
when retracting the array.
2.40 Withdraw the disposable device from the patient.
2.41 TURN OFF THE NOVASURE RF CONTROLLER.
2.42 Perform postoperative patient care according to standard
procedures.
2.43 Discharge the patient from the hospital or office as indicated by the
managing physician.
Periodic Maintenance and Service
The RF controller has been designed and tested to meet IEC 60601-1
and other safety standards. Maintenance is not required as the system
performs self-checks when power is turned on. To clean the controller
refer to the “Cleaning and Sanitizing” section.
The expected life of the RF Controller is five years or 2000 procedures
provided that damage from physical impact, such as dropping or rough
handling is avoided. If the controller is dropped or suffers severe
physical impact, discontinue use and contact Hologic technical support.
Refer to the “Technical Support and Product Return Information” section.
There is no service manual for the NovaSure RF Controller since there
are no field serviceable components within the unit.
WARNING: No modification of this equipment is allowed.
RF power output test
The NovaSure RF controller Model 10 integrates automatic power output
testing in a power on self test (POST). During the POST the controller’s
power output (Pc) is delivered into a shunt resistor (Rs) located inside
the controller. Pc is targeted to be 180 watts and Rs is nominally 25
ohms. During the POST, no power is delivered to the disposable device
connector at the front of the controller.
The NovaSure RF controller Model 10 performs POST automatically
upon power up. To access POST information, go to Settings and scroll to
System Information. Press the “View Info.” button.
NOTE: If a system fault occurs during the POST, toggle off the power
at the power input module and repeat the POST. If a system fault
occurs a second time, remove the RF controller from service and
contact Hologic Technical Support.
CAUTION: Do not attempt to repair the controller if problems are
suspected. Follow the troubleshooting guide in this manual. If
problems persist, call Hologic Technical Support for instructions.
Sterile NovaSure disposable device: No maintenance is necessary.
Single-patient use only. Do not reuse or re-sterilize the NovaSure
disposable device.
NovaSure Model 10 RF Controller Screen Icons
The following is a description of the icons on the NovaSure Model 10 RF
controller screen.
Settings Icon:
Press this button to display the
setting options for Language,
Brightness, and Volume.
Last Procedure Icon:
Press this button to display the
“Procedure Complete” Screen
and review the summary from
the last procedure.
Help Icon:
Press this button to display more information
regarding the current step of the procedure.
This icon will display an abridged version of
the IFU language.

17
ENGLISH
NOTE: When the “Last Procedure” Icon is pressed, only the previous
procedure will be displayed. Information for procedures prior to the
most recent procedure will not be available.
NOTE: In the “Settings” screen, press the “-” or “+” buttons to
adjust the volume and brightness.
NOTE: The first time the Model 10 RFC is turned on, the “Select Your
Language” screen will display. The default setting is in English. To
select another language, press the button with the name of that
language. Save the selection by pressing the flashing green button.
The language selection will be retained. To change the language
selection after the initial setup, use the “Setting” screen. Press the
name of the language to change the language used on the screen
display. To save changes to the settings, press the flashing green
button. To cancel a selection, press the blue “X”.
Troubleshooting Most Common Alarms
CAVITY ASSESSMENT ALARM
If the cavity integrity assessment fails, a screen will display “Cavity
Assessment Failure” with an abridged version of the troubleshooting tips
below. The cause of the cavity integrity assessment (CIA) failure is the
inability to pressurize the cavity. It may be caused by:
1. Device leak: Ensure that the suction line desiccant filter has been
installed. Check all tubing connections to ensure that they are tightly
connected.
2. Leak at the external os of the cervix: Look for visible bubbles or a
“hissing” sound at the external os of the cervix.
Use the tab on the cervical collar to advance the cervical collar
towards the external os of the cervix to ensure there is a tight seal.
Perform the CIA test again. If the CIA test fails again, use a second
tenaculum to grasp the cervix around the sheath of the NovaSure
disposable device. Perform the CIA test again.
3. Uterine perforation: If a perforation is suspected, the procedure
should be terminated immediately.
NOTE: CO2 leakage may occur at the external cervical os due to the
presence of an over-dilated cervix. Visible bubbles or the “hissing”
sound of escaping gas may accompany CO2 leakage under either of
these conditions.
NOTE: When following the troubleshooting steps on the Model 10
RFC, press the “?” button on the screen and use the scroll buttons
on the right for more information. To get back to the main screen
from the additional troubleshooting tips, press the “X” in the top
right corner of the screen.
If the cavity integrity assessment fails after reasonable attempts
to implement the troubleshooting procedure (step 2.36), abort the
procedure.
VACUUM ALARM
The Vacuum alarm occurs when the vacuum level is outside its specified
range. This can occur as a result of one or more of the following:
• An over-dilated cervix;
• Poor contact between the cervical collar and the external cervical os;
• The vacuum relief valve is in the closed position;
• An obstruction in the disposable device filter(s) (two) or desiccant; or
• An obstruction within the disposable device.
If the Vacuum check fails, a screen will display “Vacuum Failure” with an
abridged version of the following troubleshooting tips:
• Gently press a 2-3.5 mm uterine dilator or sound inside the vacuum
relief valve
• Check the cervical collar position, and reposition if necessary. Use the
tab on the cervical collar to advance the cervical collar towards the
external os of the cervix to ensure there is a tight seal. Verify that air is
not being drawn through the cervix by a loose fit between the cervical
collar and the entrance to the cervical canal. If air is being drawn in
through the cervical canal, try to reposition the cervical collar and
disposable device shaft to prevent air ingress.
• Ensure the suction canister on the disposable device is vertical and the
device tubing is not draped over the patient’s leg.
• Check all tubing connections to ensure that they are tightly connected.
Check the push-on tubing connectors at the desiccant tube. Replace
the desiccant if it is pink. Ensure that the filter located near the
disposable connection on the vacuum feedback line is tightened.
• Reattempt ablation.
If the “Vacuum Failure” screen displays again:
• Disconnect the disposable device from the RF controller.
• Remove the disposable device and replace with a new disposable
device.
• Reattempt the ablation with the new device.
NOTE: When following the troubleshooting steps on the Model 10
RFC, press the “?” button on the screen and use the scroll buttons
on the right for more information. To get back to the main screen
from the additional troubleshooting tips, press the “X” in the top
right corner of the screen.
If the vacuum alarm occurs with the new device, abort the procedure.
NOTE: Removing the disposable device from the uterine cavity after
completing a cavity integrity assesment will require an additional
CIA test to be performed upon disposable device re-insertion
(whether or not the CIA previously passed) prior to initiating an
ablation.
CO2 canister low or empty
A screen will display “Replace CO2” with an image of the back of the
controller. An audible tone will be generated at a rate of 1 time per

18
ENGLISH
second. Alarm messages that were present prior to the alarm will remain
in the same state during the replace CO2 event. Pressing the foot switch
will not turn off the audible alarm.
1. Replace the CO2 canister to stop the audible tone.
NOTE: It is not necessary to remove the disposable device from the
patient prior to replacing the canister.
2. Continue with the procedure.
ARRAY POSITION Alarm
The Array Position message displays when the array is not open fully.
The controller cannot perform ablation when Array Position message
displays. If the ARRAY POSITION alarm occurs, a screen will display
“Check Array” with an abridged version of the following troubleshooting
tips:
1. Gently move the proximal end of the disposable device and observe
if the Array Position message no longer displays. If it still displays,
proceed with the following:
2. Attempt gentle reseating of the NovaSure disposable device:
A. Partially retract the array into the sheath by releasing the
disposable device handle lock release button;
B. Pull the disposable device back slightly from the fundus;
C. Slowly redeploy the disposable device array while gently
rocking the disposable device back and forth and locking the
disposable device handles; and
D. Reseat the disposable device against the fundus using the
seating procedure described in steps 2.26 through 2.33.
3. If the uterus is retroverted, take special care to avoid perforation.
Apply gentle caudad traction to the cervix with the tenaculum, and
elevate the disposable device handle upward toward the ceiling
(in-line with the axis of the uterus) while performing the seating
procedure.
4. If the Array Position message still displays, fully retract the
disposable device array and remove the disposable device from the
patient.
5. Deploy the disposable device outside the patient’s body; ensure the
electrode array is undamaged and that the Array Position message
no longer displays.
6. Attempt reinsertion, redeployment and reseating of the disposable
device using the seating procedure described in section 2.0.
7. If the Array Position message still displays, replace with a new
disposable device.
8. If the Array Position message displays with a new disposable device,
terminate the procedure.
NOTE: When following the troubleshooting steps on the Model 10
RFC, press the “?” button on the screen and use the scroll buttons
on the right for more information. To get back to the main screen
from the additional troubleshooting tips, press the “X” in the top
right corner of the screen.
Please turn to next page for the
remainder of the Instructions for Use.
Additional Troubleshooting

19
ENGLISH
Suspected uterine perforation
Prior to Application of Energy:
1. Terminate the procedure
2. Assure patient stability
3. Consider work-up for
perforation
4. Reschedule procedure,
if appropriate
During or after Application of
Energy:
1. Terminate the procedure
2. Assure patient stability
3. Rule out visceral injury
4. Reschedule procedure,
if appropriate
Array does not fully deploy and lock in uterus
1. Partially retract array into sheath (hold the front handle stationary
and pull the rear handle back and away from the patient);
2. Reposition the disposable device in the cavity;
3. Redeploy the array in cavity;
4. If the disposable device does not lock, remove it from the uterus;
5. Inspect the disposable device for damage;
6. Attempt to open the disposable device and lock it outside the patient;
7. If damaged, the replace disposable device;
8. If the disposable device is not damaged, reinsert it into the patient’s
uterine cavity and attempt deployment; and
9. If unable to deploy the disposable device to a minimum 2.5cm
cornu-to-cornu distance, terminate the procedure.
10. Consider uterine perforation as a possible cause for not deploying.
Difficulty closing and removing the disposable device
post-ablation
Confirm that the lock release button is depressed:
• If so, gradually withdraw the disposable device from the patient.
• If not, press the lock release button and reattempt to close the
disposable device. If it is still difficult to close, gradually withdraw the
disposable device from the patient.
“Procedure Complete” Screen does not appear on the Model 10
RFC at the end of a procedure
If power has not been applied for at least 30 seconds, the “Procedure
Not Complete” screen will appear on the Model 10 RFC.
Procedure Not Complete
1. Remove device from patient and deploy array
a. Confirm that array is NOT damaged
b. Confirm that array Position does NOT display
2. For more help press ?
if a and b are confirmed, reinsert device, and PRESS FOOT SWITCH
to reattempt treament.
If a problem is found, replace device and restart procedure.
1. Remove the NovaSure disposable device from the uterus after fully
retracting the disposable device array into the sheath:
A. Release the disposable device lock release button;
B. Hold the disposable device front handle steady; and
C. Pull the disposable device rear handle backward.
2. Inspect the disposable device for any damage. Fully deploy the
electrode array outside the patient, demonstrating that the message
does not display on the Model 10 RFCs.
3. If the disposable device is not damaged and the message screen
does not appear on the Model 10 RFC, reinsert, redeploy and
reattempt treatment.
4. If the problem persists, replace the disposable device with a new
disposable device.
5. Reattempt the procedure. If the problem persists, terminate the
procedure.
“RF ON” screen will not appear on the Model 10 RFC
1. If the NovaSure RF controller is plugged in, switched on, the ENABLE
button has been pressed and no power is delivered from the
controller when the foot switch is depressed, check the foot switch
connection. Also make sure the CAVITY ASSESSMENT has passed.
2. If the problem persists, terminate the procedure.
UP/DOWN values will not appear when pressing the appropriate
buttons
Make sure that the disposable device is connected to the controller.
The values will not appear unless the disposable device is properly
connected to the controller.
Replacement Instructions
The NovaSure RF controller uses a pair of fuses that are located on
a fuse carrier in the power input module. Type T5AH, 250V fuses are
used. The module can be accessed by using a slotted screwdriver to
pop open the fuse carrier door. If required, the fuse carrier may then be
removed and the fuses changed. Assembly is the reverse of these steps.
Any potentially defective NovaSure product must be returned to Hologic
for evaluation. Follow the instructions at the end of this manual in the
Service Returns section, for obtaining a returned materials authorization
number (RMA #). Do not discard the NovaSure disposable device.
Technical Specifications
NovaSure disposable device
1. The NovaSure disposable device does not contain latex.
2. The NovaSure disposable device is a Class III device by FDA
regulation.
3. The NovaSure disposable device is a Class IIB device according to
the Regualtion MDD 93/42EEC.
4. The NovaSure disposable device tip nominal diameter: 6mm.
5. The NovaSure disposable device overall dimensions:
19” x 6” x 12” (48.3cm x 15.2cm x 5cm).
6. The NovaSure disposable device has a voltage rating of 153V.

20
ENGLISH
NovaSure RF controller
1. The NovaSure RF controller can be used with outlets providing 100 to
240 VAC and will draw a maximum of 5 Amps.
2. The NovaSure RF controller is a Class I, defibrillator-proof Type BF
instrument, according to IEC 60601-1.
3. The NovaSure RF controller is a Class III device by FDA regulation.
4. The NovaSure RF controller is a Class IIB device according to the
MDD 93/42EEC.
5. The RF controller has been tested and found to comply with the
limits for medical devices according to IEC 60601-1-2 ED 4.0: 2014.
These limits are designed to provide reasonable protection against
harmful interference in a typical medical installation. This equipment
generates, uses and can radiate radio frequency energy and, if not
installed and used in accordance with the instructions, may cause
harmful interference to other devices in the vicinity. However, there
is no guarantee that interference will not occur in a particular
installation. If this equipment does cause harmful interference to
other devices, which can be determined by turning the equipment off
and on, the user is encouraged to try to correct the interference by
one or more of the following measures:
• Re-orient or relocate the receiving device
• Increase the separation between equipment
• Connect the equipment into an outlet on a circuit different from that
to which the other device(s) is/are connected.
• Contact Hologic Technical Support (or the manufacturer of the other
equipment) for assistance.
6. The controller meets the requirements of IEC60601-1/UL60601-1,
IEC60601-2-2 and CSAC22.2No.601.1.
7. Shipment of the controller should be done only in the original Hologic
packaging. Environmental requirements for use, shipping and
storage are indicated below.
8. The absolute maximum peak voltage generated by the
NovaSureRFcontroller is 153volts. Accessories used with the RF
controller should have a voltage rating equal to or greater than
153volts.
9. The absolute maximum peak power generated by the
NovaSureRFcontroller is 216 watts.
10. NovaSureRFcontroller weight: 24lbs (11kg), unpacked.
11. Height: 12.5”; Width: 7.5”; Depth: 14.5”
(32cm x 19cm x 35.5cm).
12. The maximum pressure of CO2 delivered from the NovaSure
RF controller and disposable device shall be 90 ±10mmHg.
The maximum flow rate of CO2 from the NovaSure RF controller
connected to the disposable device shall be 95 ±15ml/min. (The
maximum flow rate of CO2 from the NovaSureRF controller without a
NovaSure disposable device attached is 105 - 130ml/ min.)
13. The Novasure RF Generator should be used without a neutral
electrode.
Environmental Conditions
NovaSure RF controller
Operating, non-packaged conditions
Altitude 0 to 10,000ft (0 to 3,030m)
Temperature 10°C to 40°C (50°F to 104°F)
Humidity 15 to 85% RH (non-condensing)
Non-operating, packaged conditions
Altitude 0 to 40,000 ft (0 to12,120 m)
Temperature –30°C to 60°C (–22°F to 140°F)
Humidity 85% RH, (non-condensing)
up to 90% RH, (non-condensing).
Power vs. Resistance
Measured Power (Watts)
Load Resistance (Ohms)
Actual Power vs. Power Setting into a 20 Ohm Load
Actual Power (Watts)
Power Setting (Watts)

21
ENGLISH
Important Performance Characteristics
• Air must be purged from the device for 10 seconds prior to insertion
in patient.
• The Cavity Integrity Assessment (CIA) must measure a pressure of
50 ± 10 mm of Hg for 3 seconds minimum to pass. Otherwise the
CIA will report an error. The RF controller will not enable an ablation
to begin until CIA passes.
• RF power: The range of RF power delivery is 55 to 180 (+/-20%)
watts.
• Vacuum pressure monitoring: During an ablation the vacuum
pressure must be in the range of 0.7 ±0.2 in Hg to 6 ±1.0 in Hg. If
the vacuum pressure exceeds this range, the controller will end the
ablation.
• Impedance monitoring: The RF Controller will end an ablation when
the measured tissue impedance reaches approximately 50 ohms.
• Two minute timer: After two minutes of RF energy delivery, the
controller will end the ablation
• Ten minute timeout: after completing the ablation procedure the
controller times out for 10 minutes, during which the controller is
incapable of delivering energy.
• DC Short Circuit protection: If the RF controller detects a short
circuit (i.e. <13+/-6ohms), the ablation will be ended.
Electromagnetic Safety Guidance
Table 1 - Guidance and manufacturer’s declaration –
Electromagnetic emissions
Guidance and manufacturer’s declaration – Electromagnetic emissions
The NovaSure RF controller is intended for use in the electromagnetic
environment specified below. The customer or user of the NovaSure RF
controller should ensure that it is used in such an environment.
Emissions
Test Compliance Electromagnetic Environment – Guidance
RF Emissions
CISPR 11
Group 1 The NovaSure RF controller must emit
electromagnetic energy in order to perform
its intended function. Nearby electronic
equipment may be affected.
RF Emissions
CISPR 11
Class A The NovaSure RF controller is intended for use
in Professional Healthcare Facilities including
hospitals and physician’s offices.
WARNING: The EMISSIONS characteristics
of this equipment make it suitable for use
in industrial areas and hospitals (CISPR
11 Class A). If it is used in a residential
environment (for which CISPR 11 Class
B is normally required) this equipment
might not offer adequate protection to
radio-frequency communication services.
The user might need to take mitigation
measures, such as relocating or re-
orienting the equipment.
Harmonic
emissions
IEC 61000-
3-2
Class A
Voltage
fluctuations/
flicker
emissions
IEC 61000-
3-3
Complies
WARNING: In some circumstances, the potential exists for alternate
site burns whenever a high-frequency device is used. Skin-to-skin
contact should be avoided, for example, by insertion of dry gauze.
WARNING: With any electrosurgical device, the potential for arcing
exists, and neuromuscular stimulation may occur.When this device
is used properly in the uterus, the risk of muscle stimulation,
particularly heart muscle, is remote.
Table 2 - Guidance and manufacturer’s declaration –
Electromagnetic immunity
Guidance and manufacturer’s declaration – Electromagnetic immunity
The NovaSure RF controller is intended for use in the electromagnetic
environment specified below. The customer or user of the NovaSure RF
controller should ensure that it is used in such an environment.
Immunity
Test IEC 60601
Test Level Compliance
Level Electromagnetic
Environment – Guidance
Electrostatic
discharge
(ESD)
IEC 61000-
4-2
±2kV,
±4kV, ±8kV
Contact
±2kV, ±4kV,
±8kV Contact
Floors should be wood,
concrete or ceramic tile.
If floors are covered with
synthetic material, the relative
humidity should be at least
30%.
±2kV, ±4kV,
±8kV, ±15kV
Air
±2kV, ±4kV,
±8kV,±15kV
Air
Electrical
fast
transient/
burst
IEC 61000-
4-4
±0.5kV, ±1kV,
±2kV for
power supply
lines
100kHz
repetition
frequency
±0.5kV, ±1kV,
±2kV for
power supply
lines
100kHz
repetition
frequency
Mains power quality should be
that of a typical commercial or
hospital environment.
Surge
IEC 61000-
4-5
±0.5kV,
±1kV line(s)
to line(s)
±0.5kV,
±1kV line(s)
to line(s)
Mains power quality should be
that of a typical commercial or
hospital environment.
±0.5kV, ±1kV,
±2kV line(s)
to earth
±0.5kV, ±1kV,
±2kV line(s)
to earth

22
ENGLISH
Guidance and manufacturer’s declaration – Electromagnetic immunity
The NovaSure RF controller is intended for use in the electromagnetic
environment specified below. The customer or user of the NovaSure RF
controller should ensure that it is used in such an environment.
Immunity
Test IEC 60601
Test Level Compliance
Level Electromagnetic
Environment – Guidance
Voltage
dips, short
interuptions,
and voltage
variations
on power
supply input
lines
IEC 61000-
4-11
0 % UT ; 0.5
cycle At 0°,
45°, 90°,
135°, 180°,
225°, 270°
and 315°
0 % UT ; 0.5
cycle At 0°,
45°, 90°,
135°, 180°,
225°, 270°
and 315°
Mains power quality should be
that of a typical commercial
or hospital environment. If
the user of the NovaSure
RF controller requires
continued operation during
power mains interruptions,
it is recommended that
the NovaSure RF controller
be powered from an
uninterruptible power supply
or battery.
0 % UT; 1
cycle and
70 % UT ;
25/30 cycles
Single phase:
at 0°
0 % UT; 1
cycle and
70 % UT ;
25/30 cycles
Single phase:
at 0°
0 % UT ; 250
cycles
0 % UT ; 250
cycles
This condition
causes the
RF controller
to shut
down and
then return
to standby
mode.
Power
Frequency
50/60Hz
Magnetic
Field
IEC 61000-4-8
30 A/m
50 Hz
30 A/m
50 Hz
Power frequency magnetic
fields should be that of a
typical commercial or hospital
environment.
NOTE: UT is the a.c. mains voltage prior to application of the test level.
Table 3 - Guidance and manufacturer’s declaration –
Electromagnetic immunity
Guidance and manufacturer’s declaration – Electromagnetic
immunity
The NovaSure RF controller is intended for use in the electromagnetic
environment specified below. The customer or user of the NovaSure RF
controller should ensure that it is used in such an environment.
Immunity
Test IEC
60601
Test
Level
Compliance
Level Electromagnetic Environment
– Guidance
Conducted
RF
IEC 61000-
4-6
3 V
0.15 MHz
- 80 MHz
6 V in
ISM and
amateur
radio bands
between
0.15 MHz
and 80
MHz
80% AM at
1 kHz
3 V
0.15 MHz - 80
MHz
6 V in ISM
and amateur
radio bands
between
0.15 MHz and
80 MHz
80% AM at 1
kHz
Portable RF communications
equipment (including peripherals
such as antenna cables and
external antennas) should be
used no closer than 30 cm
(12 inches) to any part of the
NovaSure Impedance Controlled
Endometrial Ablation System,
including cables specified
by Hologic Inc. Otherwise,
degradation of the performance
of this equipment could result.
Field strengths from fixed RF
transmitters, as determined
by an electromagnetic site
survey,a a should be less than
the compliance level in each
frequency rangeb.
Interference may occur in the
vicinity of equipment marked
with the following symbol:
Radiated
RF
IEC 61000-
4-3
3 V/m
80 MHz -
2.7GHz
80% AM
at 1 kHz
3 V/m
80 MHz -
2.7GHz
80% AM at
1 kHz
NOTE 1: At 80 MHz and 800 MHz, the higher frequency range applies.
NOTE 2: These guidelines may not apply in all situations.
Electromagnetic propagation is affected by absorption and reflection
from structures, objects and people.
a Field strengths from fixed transmitters, such as base stations for radio (cellular/cordless) telephones
and land mobile radios, amateur radio, AM and FM radio broadcast and TV broadcast cannot be predicted
theoretically with accuracy. To assess the electromagnetic environment due to fixed RF transmitters, an
electromagnetic site survey should be considered. If the measured field strength in the location in which
the RF generator is used exceeds the applicable RF compliance level above, the RF generator should be
observed to verify normal operation. If abnormal performance is observed, additional measures may be
necessary, such as re-orienting or relocating the RF generator.
b Over the frequency range 150 kHz to 80 MHz, field strengths should be less than 3 V/m.

23
ENGLISH
Recommended separation distances between portable
and mobile RF communications equipment and the
NovaSureRFcontroller
Portable RF communications equipment (including peripherals such as
antenna cables and external antennas) should be used no closer than
30 cm (12 inches) to any part of the NovaSure Impedance Controlled
Endometrial Ablation System, including cables specified by Hologic Inc.
Otherwise, degradation of the performance of this equipment could
result.
Cleaning and Sanitizing
The use of nonflammable agents for cleaning and sanitizing is
recommended. Flammable agents or solvents for cleaning or sanitizing
should be allowed to evaporate before use of the NovaSure system.
Portable RF communications equipment (including peripherals such as
antenna cables and external antennas) should be used no closer than
30 cm (12 inches) to any part of the NovaSure Impedance Controlled
Endometrial Ablation System, including cables specified by Hologic Inc.
Otherwise, degradation of the performance of this equipment could
result.
The NovaSure RF controller is not sterile. Cleaning should be done using
a mild detergent and water solution to wipe surface areas only. Do not
immerse unit in liquid or introduce liquid into the cooling vents or RF
cable areas.
The NovaSure disposable device is a sterile disposable device for single-
patient use only.
• Do not use if the packaging is opened or damaged.
• Do not reuse or re-sterilize the disposable device.
Do not sterilize any component of the NovaSure impedance controlled
endometrial ablation system.
Parts List
Ordering information and related parts and accessories
Product Number Description
RFC2010 NovaSure RF Controller, Model 10
814002 Power Cord, 115 Volts, North America
814003 Power Cord, 230 Volts, Europe
814004 Power Cord, 220 Volts, United Kingdom/Ireland
814005 Power Cord, Denmark
814009 Power Cord, Italy
814011 Power Cord, Switzerland
814015 Power Cord, Japan
814016 Power Cord, Australia
52124-001 Foot Switch
815012 CO2 (USP), Cylinder 5 Pack
NS2013 NovaSure Impedance Controlled Endometrial
Ablation Disposable Device Kit
300001 Biohazard Kit
Disposal
CAUTION: The used disposable device must be treated as
biohazardous waste and disposed of according to standard
practices of the hospital or clinic where the treatment is
performed.
Hologic and its distributors and customers in the European Community
are required to comply with the Waste Electrical and Electronic
Equipment (WEEE) Directive (2002/96/EC). Hologic is dedicated to
meeting country specific requirements related to the environmentally
sound treatment of its products. Hologic’s objective is to reduce
the waste resulting from the disposal of its electrical and electronic
equipment. Hologic realizes the benefits of subjecting such WEEE to
potential reuse, treatment, recycling or recovery to minimize the amount
of hazardous substances entering the environment. Hologic customers
in the European Community are responsible for ensuring that medical
devices marked with the following symbol, indicating that the WEEE
Directive applies, are not placed into a municipal waste system unless
authorized to do so by local authorities.
Contact Hologic Technical Support to arrange for proper disposal of the
RF controller in accordance with the WEEE Directive.
Warranty
Except as otherwise expressly stated in the Agreement: i) Equipment
manufactured by Hologic is warranted to the original Customer
to perform substantially in accordance with published product
specifications for one (1) year starting from the date of shipment, or if
Installation is required, from the date of Installation (“Warranty Period”);
ii) digital imaging mammography x-ray tubes are warranted for twenty-
four (24) months, during which the x-ray tubes are fully warranted for the
first twelve (12) months and are warranted on a straight-line prorated
basis during months 13-24; iii) replacement parts and remanufactured
items are warranted for the remainder of the Warranty Period or ninety
(90) days from shipment, whichever is longer; iv) consumable Supplies
are warranted to conform to published specifications for a period
ending on the expiration date shown on their respective packages;
v) licensed Software is warranted to operate in accordance with
published specifications; vi) Services are warranted to be supplied in
a workman-like manner; vii) non-Hologic Manufactured Equipment is
warranted through its manufacturer and such manufacturer’s warranties
shall extend to Hologic’s customers, to the extent permitted by the
manufacturer of such non-Hologic Manufactured Equipment. Hologic
does not warrant that use of Products will be uninterrupted or error-free,
or that Products will operate with non-Hologic authorized third-party
products.
These warranties do not apply to any item that is: (a) repaired, moved, or
altered other than by Hologic authorized service personnel; (b) subjected
to physical (including thermal or electrical) abuse, stress, or misuse;
(c) stored, maintained, or operated in any manner inconsistent with
applicable Hologic specifications or instructions, including Customer’s
refusal to allow Hologic recommended Software upgrades; or (d)

24
ENGLISH
designated as supplied subject to a non-Hologic warranty or on a pre-
release or “as-is” basis.
Technical Support and Product Return Information
WARNING: Dropping the RF controller voids the warranty and could
damage the controller beyond repair. We strongly recommend a
stable cart which includes strapping or stabilizing the controller
to reduce the risk of being dropped. Please use extra care if
transporting the RF controller to an off-site facility. If you have any
questions regarding the RF controller, please call 1-800-442-9892
or (508) 263-2900.
Service representatives
Should the NovaSure RF controller become inoperable, contact Hologic
Technical Support for instructions and a return materials authorization
number (RMA#). Clean and repackage the controller appropriately and
return it for repair or servicing to the authorized locations listed below. If
the controller is not under warranty, an appropriate handling and repair
charge will be established at receipt and examination of the NovaSure
RF controller.
For More Information
For Technical Support or reorder information in the United States,
please contact:
Hologic, Inc.
250 Campus Drive
Marlborough, MA 01752 USA
Phone: 800-442-9892 (toll-free)
www.hologic.com
NOTE: Any incident or problem, which is believed to represent a
safety issue, should be reported to Hologic Technical Support.
International customers, contact your distributor or local Hologic Sales
Representative:
Hologic BV
Da Vincilaan 5
1930 Zaventem
Belgium
Tel: +32 2 711 46 80
Fax: +32 2 725 20 87
Report any complaints or problems in the quality, reliability, safety,
or performance of this product to Hologic. If the device has caused
or added to patient injury, immediately report the incident to Hologic
Authorized Representative and Competent authority of the respective
member state or country. The Competent Authorities, for medical
devices, are usually the individual Member States’ Ministry of Health, or
an agency within the Ministry of Health.
Service returns
Read these instructions prior to returning any used/unused
potentially defective product to Hologic.
Contact Hologic Technical Support if the NovaSure disposable device or
RF controller fails to operate as intended. If product is to be returned to
Hologic for any reason, Technical Support will issue a Returned Materials
Authorization (RMA) number and biohazard kit if applicable.
Return RF controllers according to the instructions provided by Technical
Support. Be sure to clean the RF controller before returning it and include
all accessories in the box with the returned unit.
Return used or opened disposable devices according to the instructions
provided with the Hologic-supplied biohazard kit.

25
ENGLISH
Symbol Glossary
Symbol Standard Refer-
ence & Symbol
Number Title of Symbol Description of Symbol
REPEC
EN ISO 15223-1,
5.1.2
Authorized
representative
in the European
Community
Indicates the Authorized
representative in the
European Community.
IEC 60601-1,
Table D.1, 1
IEC 60417, 5032
Alternating cur-
rent (AC)
To indicate on the
rating plate that the
equipment is suitable
for alternating current
only; to identify relevant
terminals.
EN ISO 15223-1,
5.3.9
ISO 7000, 2621
Atmospheric
pressure limita-
tion
Indicates the range of
atmospheric pressure
to which the medical
device can be safely
exposed.
EN ISO 15223-1,
5.1.5
ISO 7000, 2492 Batch code
Indicates the manufac-
turer’s batch code so
that the batch or lot can
be identified.
CO2N/A Carbon dioxide Indicates carbon
dioxide.
EN ISO 15223-1,
5.1.6
ISO 7000, 2493
Catalogue num-
ber
Indicates the manufac-
turer’s catalogue num-
ber so that the medical
device can be identified.
N/A Category non-
AP equipment To identify category
non-AP equipment.
EN ISO 15223-1,
5.4.4
ISO 7000, 0434A
IEC 60601-1,
Table D.1, 10
Caution
To indicate that cau-
tion is necessary when
operating the device or
control close to where
the symbol is placed,
or to indicate that the
current situation needs
operator awareness or
operator action in order
to avoid undesirable
consequences.
European
Medical Direc-
tive 93/42/EEC,
Article 17 and
Annex XII
European Medi-
cal Device Regu-
lation 2017/745,
Annex V
CE marking of
conformity
with notified
body identifica-
tion number
Indicates the medi-
cal device conforms
to European Medical
Directive 93/42/EEC and
meets applicable health,
safety, and environmen-
tal requirements. If the
mark is accompanied by
a number, conformity is
verified by the indicated
notified body.
EN ISO 15223-1,
5.4.3
ISO 7000, 1641
IEC 60601-1,
Table D.1, 11
Consult instruc-
tions for use
Indicates the need for
the user to consult the
instructions for use.
Symbol Standard Refer-
ence & Symbol
Number Title of Symbol Description of Symbol
CC
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 6049
Country of
manufacture
To identify the country
of manufacture of
products
IEC 60601-1,
Table D.1, 24
IEC 60417, 5036
Dangerous volt-
age
To indicate hazards
arising from dangerous
voltages.
EN ISO 15223-1,
5.1.3
ISO 7000, 2497
Date of manu-
facture
Indicates the date when
the medical device was
manufactured.
IEC 60601-1,
Table D.1, 26
IEC 60417, 5334
Defibrillator-
proof Type BF
equipment
To identify a defibril-
lation-proof type BF
applied part complying
with IEC 60601-1.
EN ISO 15223-1,
5.2.6
ISO 7000, 2608
Do not resteril-
ize
Indicates a medical
device that is not to be
resterilized.
EN ISO 15223-1,
5.4.2
ISO 7000, 1051
IEC 60601-1,
Table D.1, 28
Do not re-use Indicates a medical
device that is intended
for one single use only.
ISO 7000, 2403
ISO 780 Do not stack
above “n” high
To indicate that the
items shall not be verti-
cally stacked beyond
the specified number,
either because of the
nature of the transport
packaging or because
of the nature of the
items themselves.
EN ISO 15223-1,
5.2.8
ISO 7000, 2606
Do not use if
package is
damaged
Indicates a medical
device that should not
be used if the package
has been damaged or
opened and that the
user should consult the
instructions for use for
additional information.
IEC 60601-1,
Table D.1, 8
IEC 60417, 5021
Equipotential
ground
To identify the terminals
which, when connected
together, bring the vari-
ous parts of an equip-
ment or of a system to
the same potential, not
necessarily being the
earth (ground) potential,
e.g. for local bonding.
WEEE Directive
2002/96/EC
2012/19/EC
EN 60417, 6414
European Com-
munity Waste
Electrical and
Electronic
Equipment
(WEEE) Directive
2002/96/EC
To indicate that sepa-
rate collection for waste
electric and electronic
equipment (WEEE) is
required.

26
ENGLISH
Symbol Standard Refer-
ence & Symbol
Number Title of Symbol Description of Symbol
IEC 60417, 5114 Foot switch To identify a foot switch
or the connection for a
foot switch.
ISO 7010
ISO 3864-2,
M002
Follow instruc-
tions for use
To signify that the in-
struction manual/book-
let must be read.
EN ISO 15223-1,
5.3.1
ISO 7000, 0621
ISO 780
Fragile
Indicates a medical
device that can be bro-
ken or damaged if not
handled carefully.
IEC 60143-1,
5016 Fuse To identify fuse boxes or
their location.
HP N/A High pressure Indicates high pressure.
EN ISO 15223-1,
5.3.8
ISO 7000, 2620
Humidity limita-
tion
Indicates the range of
humidity to which the
medical device can be
safely exposed.
EN ISO 15223-1,
5.3.2
ISO 7000, 0624
ISO 780
Keep away from
heat
Indicates a medical de-
vice that needs protec-
tion from heat sources.
EN ISO 15223-1,
5.3.4
ISO 7000, 0626
ISO 780
Keep dry
Indicates a medical
device that needs to be
protected from mois-
ture.
EN ISO 15223-1,
5.1.1
ISO 7000, 3082 Manufacturer Indicates the medical
device manufacturer
ISO/DIS 15223-
1, 5.7.7 Medical device Indicates the item is a
medical device
N/A No oil Indicates no oil.
EN ISO 15223-1,
5.1.7
ISO 7000, 2609 Non-sterile
Indicates a medical de-
vice that has not been
subjected to a steriliza-
tion process.
LATEX EN ISO 15223-1,
Annex B
Not made with
natural rubber
latex
Indicates no presence
of dry natural rubber or
natural rubber latex.
ISO 7000, 2794 Packaging unit To indicate the number
of pieces in the pack-
age.
FDA 21 CFR 801 Prescription use
only
Caution: Federal law
restricts this device to
sale by or on the order
of a physician.
Symbol Standard Refer-
ence & Symbol
Number Title of Symbol Description of Symbol
IEC 60417, 5140 Non-ionizing
electromagnetic
radiation
To indicate generally
elevated, potentially
hazardous, levels of
non-ionizing radiation,
or to indicate equip-
ment or systems e.g. in
the medical electrical
area that include RF
transmitters or that
intentionally apply RF
electromagnetic energy
for diagnosis or treat-
ment.
EN ISO 15223-1,
5.1.7
ISO 7000, 2498 Serial number
Indicates the manufac-
turer’s serial number so
that a specific medical
device can be identified.
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 3707
Single sterile
barrier system Indicates a single sterile
barrier system
EN ISO 15223-1,
5.2.3
ISO 7000, 2501
Sterilized using
ethylene oxide
Indicates a medical
device that has been
sterilized using ethylene
oxide.
EN ISO 15223-1,
5.3.7
ISO 7000, 0632
Temperature
limit
Indicates the tempera-
ture limits to which the
medical device can be
safely exposed.
ISO 7000, 0623
ISO 780, 0623
IATA 2004 This side up To indicate correct
upright position of the
transport package.
UDI
ISO/DIS 15223-
1, 5.7.10 Unique Device
Identifier
Indicates a carrier that
contains Unique Device
Identifier information
EN ISO 15223-1,
5.1.4
ISO 7000, 2607 Use-by date Indicates the date after
which the medical de-
vice is not to be used.
Hologic, NovaSure and associated logos are trademarks and/or
registered trademarks of Hologic, Inc. and/or its subsidiaries in the
UnitedStates and/or other countries.
The NovaSure impedance controlled endometrial ablation system is
manufactured and distributed by Hologic, Inc.
© 2014-2022 Hologic, Inc.
AW-22724-001 Rev. 001
04/2022

1
NEDERLANDS
NovaSure®
Gebruiksaanwijzing en handleiding voor de
regelaar
Inhoudsopgave
Checklist voor de arts ......................................1
Beschrijving van het systeem ................................1
Indicaties ................................................3
Patiëntendoelgroep ........................................3
Beoogde klinische voordelen voor patiënten .....................3
Beoogde gebruiker .........................................3
Contra-indicaties ..........................................3
Waarschuwingen ..........................................4
Voorzorgsmaatregelen ......................................5
Klinische gegevens inzake NovaSure over een 3-jarige periode ........6
Ongewenste voorvallen ...................................6
Mogelijke postprocedurele complicaties .....................7
Andere ongewenste voorvallen ............................. 7
Klinisch onderzoek ......................................7
Patiënten selecteren ....................................10
Patiënten begeleiden ...................................10
Voorbehandeling van de patiënt. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Gebruiksaanwijzing NovaSure endometriumablatiesysteem
metimpedantieregeling
.....................................11
Besturing van RF-regelaar model 10 .......................16
Periodiek onderhoud en service:
RF-regelaar model 10 ..................................17
Schermpictogrammen NovaSure RF-regelaar model 10 .......... 18
Problemen oplossen – de meest voorkomende alarmen:
RF-regelaar model 10 ...................................18
Instructies voor vervanging van onderdelen ....................20
Technische specificaties ...................................21
NovaSure disposable werkset ............................21
NovaSure RF-regelaar ..................................21
Omgevingsomstandigheden ..............................22
Belangrijke prestaties Kenmerken .........................22
Elektromagnetische veiligheidsrichtlijnen ...................22
Reinigen en desinfecteren ...............................24
Onderdelenlijst ........................................24
Afvoer ..................................................25
Garantie ................................................25
Technische ondersteuning en informatie over productretournering ....25
Verklaring van symbolen ...................................26
LET OP: KRACHTENS DE FEDERALE WETGEVING (VS) MAG DIT TOESTEL
SLECHTS WORDEN VERKOCHT DOOR OF IN OPDRACHT VAN EEN ARTS
MET DE JUISTE TRAINING VOOR DE BEDIENING VAN DIT HULPMIDDEL.
Lees alle instructies, voorzorgsmaatregelen en waarschuwingen
alvorens het product te gebruiken. Indien aanwijzingen,
waarschuwingen of voorzorgsmaatregelen worden genegeerd,
kanernstig letsel van de patiënt daarvan het gevolg zijn.
Opmerking: De bij de disposable werkset meegeleverde
handleiding kan een recentere versie van de instructies voor het
NovaSuresysteem bevatten dan de bij de regelaar meegeleverde
handleiding.
De NovaSuredisposable werkset mag niet worden gebruikt in
combinatie met andere RF-regelaars en/of RF-generatoren, en de
NovaSureRF-regelaar mag evenmin met andere disposable werksets
worden gebruikt.
De NovaSure disposable werkset bevat geen latex.
Checklist voor de arts
De arts moet:
• voldoende ervaring hebben met het uitvoeren van procedures binnen
de uterusholte, zoals het inbrengen van intra-uteriene anticonceptiva
of dilatatie en curettage (D&C). Ook moet hij/zij beschikken over een
adequate opleiding, kennis en routine ten aanzien van het gebruik van
het NovaSure systeem;
• de instructies bestuderen en die zich eigen maken, en de
producttraining van NovaSure voltooien of zich laten opleiden door een
daartoe bevoegd arts;
• op de hoogte zijn van de juiste volgorde van handelingen zoals beschreven
in de paragrafen 'Gebruiksaanwijzing' en 'Problemen oplossen' van
deze handleiding, zodat de behandeling kan worden onderbroken en na
oplossing van het probleem hervat indien het systeem tijdens de 'Cavity
Integrity Assessment' (CIA, beschadigingscontrole uteruswand) CO
2
-verlies
detecteert; dit kan duiden op uterusperforatie.
Ook assisterende medewerkers moeten van deze instructies en ander
voorlichtingsmateriaal op de hoogte zijn voordat zij het NovaSure systeem
in de praktijk gebruiken.
Beschrijving van het systeem
Het NovaSure endometriumablatiesysteem met impedantieregeling bestaat
uit de NovaSure disposable werkset met verbindingskabel, de NovaSure
RF-regelaar (regelaar), de NovaSure CO2-canister, een ontvochtiger, een
voetpedaal en een voedingsnetsnoer. Deze componenten worden in
onderlinge samenhang als een systeem gebruikt.
NovaSure disposable werkset met verbindingskabel,
inclusief afzuigslangontvochtiger

2
NEDERLANDS
Beschrijving van de NovaSure disposable werkset
De NovaSure disposable werkset bestaat uit een modelleerbare
tweepolige elektrodeset voor eenmalig gebruik, gemonteerd op een
uitvouwbaar frame. Hiermee kan op het gehele binnenoppervlak
van de uterusholte een confluente laesie tot stand worden gebracht.
De disposable werkset wordt transcervicaal in de uterusholte
ingebracht en vervolgens wordt de schacht teruggetrokken, zodat
de tweepolige elektrodeset in de uterusholte kan worden geplaatst
en naar de vorm van de holte kan worden gemodelleerd.
De tweepolige elektrodeset is vervaardigd van een poreus,
met een metaallaagje bekleed materiaal, waardoorheen
constant stoom en vocht vanuit het gedehydreerde weefsel
wordt opgezogen. De disposable werkset werkt in combinatie
met een daarvoor bestemde NovaSure RF-regelaar. Door deze
gecombineerde werking kan binnen gemiddeld ca. 90seconden
een patiëntspecifieke algehele endometriumablatie worden
uitgevoerd, zonder de noodzaak van gelijktijdige hysteroscopische
visualisatie of voorbehandeling van het endometrium. Door de
speciale configuratie van de tweepolige elektrodeset en het
vooraf ingestelde vermogen van de regelaar kan een regelbare
ablatiediepte in utero worden ingesteld met een sonderingsdiepte
tot 10cm en een cornu-tot-cornu-afstand van minstens 2,5cm.
Tijdens het ablatieproces wordt het endometrium door de
doorstroming van radiofrequentie-energie (RF-energie) verdampt
en/of gecoaguleerd (ongeacht de dikte van het endometrium), en
wordt het onderliggende myometriumoppervlak gedehydreerd en
gecoaguleerd.
Op grond van de afmetingen van de uterus berekent de regelaar
automatisch de optimale vermogensinstelling (W) die voor
de behandeling van de uterusholte gewenst is. Wanneer de
weefselvernietiging de optimale diepte bereikt, veroorzaakt de
toenemende weefselimpedantie automatische stopzetting van
de stroomafgifte door de regelaar. Er is dus sprake van een
zelfregulerend proces. Door continue automatische afzuiging
worden bloed, zoutoplossing en andere vloeistoffen die zich tijdens
de procedure in de uterusholte bevinden, afgevoerd.
De disposable werkset is met de regelaar verbonden door
een kabelset die bestaat uit de RF-kabel, de afzuigslang voor
drukbewaking tijdens de 'Cavity Integrity Assessment'-cyclus en
voor afzuiging tijdens de ablatiecyclus, en de vacuümretourslang
die bestemd is voor de afgifte van kooldioxide tijdens de 'Cavity
Integrity Assessment'-cyclus en voor vacuümbewaking tijdens
deablatiecyclus. Het disposable hulpmiddel is gesteriliseerd met
ethyleenoxide (EO).
Beschrijving van de NovaSure RF-regelaar
De NovaSure RF-regelaar is een generator met constante
vermogensoutput, met een nominale maximum vermogensafgifte van
180 watt. De regelaar berekent automatisch de vermogensoutput op
basis van de lengte van de uterusholte (sondemeting minus de lengte
van het endocervicale kanaal) en van de breedteafmetingen die door de
gebruiker op de regelaar worden ingetoetst. Door continue meting van de
weefselimpedantie tijdens het ablatieproces wordt de endomyometriale
ablatiediepte automatisch geregeld. De NovaSure-procedure beëindigt
zichzelf zodra de endometriale verdamping en oppervlakkige myometriale
uitdroging ongeveer 50 ohm impedantie hebben bereikt op de plaats
waar het weefsel en de elektrode met elkaar in contact staan of wanneer
de behandelingstimer twee minuten bereikt. In de regelaar is het 'Cavity
Integrity Assessment'-systeem (CIA) geïntegreerd. Hiermee wordt
gecontroleerd of er sprake is van perforatie of een ander defect in de
uteruswand. Na plaatsing van de disposable werkset in de uterusholte
wordt via de vacuümretourslang in het centrale lumen van de disposable
werkset CO2 in de holte gevoerd, bij een veilige flowsnelheid en druk.
Wanneer de CO2-druk in de holte slechts kortstondig in stand blijft (een
teken dat de uterusholte intact is), laat de CIA toe dat de NovaSure RF-
regelaar wordt ingeschakeld en wordt de behandelingsfase voortgezet.
Door een vacuümpomp in de NovaSure RF-regelaar wordt tijdens de
gehele endometriumablatieprocedure een vacuüm in de uterusholte tot
stand gebracht en in stand gehouden. Nadat het vacuüm gestabiliseerd
is, wordt het vacuümniveau gecontroleerd tijdens het vervolg van het
ablatieproces.
NovaSure RF-regelaar
model 10

3
NEDERLANDS
Beschrijving van de NovaSure
afzuigslangontvochtiger
De NovaSure afzuigslangontvochtiger
is een niet-steriele component voor
eenmalig gebruik die door de gebruiker
als slangonderdeel in de afzuigslang
wordt aangebracht voordat de
disposable werkset op de NovaSure
RF-regelaar wordt aangesloten. Tijdens
de ablatieprocedure absorbeert de
ontvochtiger het vocht dat via de
afzuigslang uit de uterusholte wordt
verwijderd.
Beschrijving van het NovaSure
voetpedaal
Het NovaSure voetpedaal is een
pneumatische schakelaar die is
aangesloten op het voorpaneel van
de NovaSureRF-regelaar. Met het
voetpedaal wordt de NovaSure RF-
regelaar in werking gesteld. Het pedaal
bevat geen elektrische componenten.
Beschrijving van de NovaSure
CO2 -canister
De NovaSure CO2-canister is een
CO2-tankje (USP) met een gewicht
van 16 gram. De canister wordt op de
regelaar op het achterpaneel van de
NovaSureRF-regelaar aangesloten
voordat de regelaar op de netvoeding
wordt aangesloten. Met het CO2-gas
wordt de uterusholte door het 'Cavity
Integrity Assessment'-systeem onder
druk gebracht.
De CO2 container met onderdeelnr.:
815012 bevat 99% CO2.
Beschrijving van het NovaSure
wisselstroomnetsnoer
Met het NovaSure wisselstroomnetsnoer,
een voedingskabel van medische
kwaliteit, wordt de NovaSure RF-
regelaar op een netvoedingsbron van
geschikte spanning aangesloten. De
voedingsaansluiting voor het netsnoer,
de netvoedingsmodule, bevindt zich op
het achterpaneel van de NovaSure RF-
regelaar.
Indicaties
Het NovaSure systeem heeft als doel het ablateren van de endometriale
bekleding van de uterus bij premenopauzale vrouwen bij wie
zwangerschap niet meer voor de hand ligt en die lijden aan menorragie
(overmatige bloeding) met benigne oorzaken.
Patiëntendoelgroep
Het NovaSure-systeem is bedoeld voor vrouwen in de premenopauze
met menorragie (zware bloedingen) vanwege goedaardige oorzaken die
geen kinderen meer willen krijgen.
Beoogde klinische voordelen voor patiënten
De bloedingen van vrouwen in de premenopauze met hevige menstruele
bloedingen vanwege goedaardige oorzaken die geen kinderen meer
willen krijgen, verminderen of stoppen.
Beoogde gebruiker
Het NovaSure-systeem moet worden gebruikt onder toezicht en
begeleiding van een verloskundig/gynaecologisch arts of een
gynaecologisch arts of chirurg. Het NovaSure-apparaat dient
hoofdzakelijk door de arts te worden bediend en de arts kan instructies
geven over de bediening van de RF-controller aan de assistent en de
controller activeren met de voetschakelaar. De RF-controller wordt
bediend door een assistent in niet-steriele uitrusting.
De arts moet:
• voldoende ervaring hebben met het uitvoeren van procedures in de
baarmoederholte, zoals het inbrengen van een spiraaltje of dilatatie
en curettage (D&C), en moet voldoende training in, kennis van en
vertrouwdheid met het gebruik van het NovaSure-systeem hebben.
• de instructies lezen, er vertrouwd mee zijn en de NovaSure-training
voltooien of door een bevoegd arts worden opgeleid.
Aanvullend personeel moet vertrouwd zijn met de gebruiksaanwijzing en
ander trainingsmateriaal voordat ze het NovaSure-systeem gebruiken.
Contra-indicaties
Het NovaSure endometriumablatiesysteem met impedantieregeling is
gecontra-indiceerd voor gebruik bij de volgende categorieën patiënten:
• Zwangere patiënten of patiënten die in de toekomst nog zwanger
willen worden. Zwangerschap na ablatie kan zowel voor de
moeder als voor de foetus gevaarlijk zijn.
• Patiënten bekend met of met vermoedelijke endometriumcarcinoom
(uteruskanker) of premaligne aandoeningen van het endometrium,
zoals niet-verholpen adenomateuze hyperplasie.
• Patiënten met omstandigheden van anatomische (bv. voorgeschiedenis
van eerder uitgevoerde klassieke keizersnede of transmurale
myomectomie) of pathologische aard (bv. langdurige medische
behandelingen) die verzwakking van het myometrium tot gevolg
kunnen hebben.
• Patiënten die ten tijde van de (voorziene) procedure lijden aan
actieve infectie van het urogenitale stelsel (bv. cervicitis, vaginitis,
endometritis, salpingitis of cystitis).

4
NEDERLANDS
• Patiënten bij wie een intra-uterien anticonceptivum is geplaatst.
De aanwezigheid van een intra-uterien anticonceptivum in de
uterusholte kan een belemmering vormen voor een NovaSure procedure.
• Patiënten bij wie de lengte van de uterusholte minder is dan 4cm.
De minimale lengte van de elektrodeset is 4cm. Het behandelen van
een uterusholte korter dan 4cm heeft verbrandingsletsel van het
endocervicale kanaal tot gevolg.
• Patiënten bij wie de uterusholte smaller is dan 2,5cm, bij meting met
de 'WIDTH' (breedte)-meetschijf van de disposable werkset nadat de
werkset is geplaatst.
• Patiënten met een actieve inflammatoire bekkenaandoening.
Waarschuwingen
Indien aanwijzingen, waarschuwingen of voorzorgsmaatregelen
worden genegeerd, kan ernstig letsel van de patiënt daarvan het
gevolg zijn.
De NovaSure disposable werkset mag alleen in combinatie met de
NovaSure RF-regelaar worden gebruik.
De beoogde behandelingsdoelstelling van de NovaSure procedure is
eenmalige uitvoering tijdens één enkele operatie. Wanneer tijdens
één operatiesessie meerdere therapiecycli met het NovaSure
systeem worden uitgevoerd, kan dat verbrandingsletsel tot gevolg
hebben.
Uterusperforatie
• Ga bij sonderen, dilateren en bij het inbrengen van de disposable
werkset voorzichtig te werk, om perforatie van de uteruswand te
voorkomen.
• Als de disposable werkset moeilijk in het cervixkanaal kan worden
ingebracht, moet op grond van klinisch inzicht worden bepaald of
verdere dilatatie gewenst is.
• Het NovaSure systeem beoordeelt middels een 'Cavity Integrity
Assessment' (CIA) of de uterusholte onbeschadigd is, en geeft voor
aanvang van de behandeling een geluidsalarm af als er kans bestaat
op perforatie (stap 2.36). (Hoewel de test als doel heeft perforaties
van de uteruswand te detecteren, is dit slechts een indicatie.
Mogelijk detecteert de CIA niet alle perforaties onder alle denkbare
omstandigheden. Klinische beoordeling blijft altijd noodzakelijk.)
• Bij vermoeden van uterusperforatie moet de procedure onmiddellijk
worden beëindigd.
• Wanneer de 'Cavity Integrity Assessment' na redelijke pogingen om
de probleemoplossingsprocedures (stap 2.36) te implementeren
geen resultaat oplevert, moet de procedure worden stopgezet.
• Voor patiënten bij wie de procedure op grond van verdenking van
perforatie van de uteruswand is afgebroken, moet aanvullende
behandeling van de perforatie worden overwogen voordat de patiënt
wordt ontslagen.
Algemeen
• Endometriumablatie met het NovaSure systeem is geen
sterilisatieprocedure. Daarom moet de patiënt worden voorgelicht
overgeschikte geboortebeperkingsmethoden.
• Door endometriumablatie wordt het risico van endometriumhyperplasie of
adenocarcinoom van het endometrium niet opgeheven, en de behandeling
kan het diagnosticeren van dergelijke aandoeningen voor de arts
bemoeilijken.
• Endometriumablatie is alleen bedoeld voor vrouwen zonder kinderwens,
aangezien de kans op zwangerschap na de procedure aanzienlijk zal
zijn verminderd. Zwangerschap na ablatie kan zowel voor de moeder als
voor de foetus gevaarlijk zijn.
• Patiënten die endometriumablatie ondergaan nadat zij al eerder met
tubaligatie zijn behandeld, lopen een verhoogde kans op post-ablatie
tubair sterilisatiesyndroom, waarbij hysterectomie noodzakelijk kan
zijn. Dit risico kan zich tot 10jaar na de procedure concretiseren.
• Er kunnen gezondheidsrisico's bestaan wanneer de NovaSure
procedure wordt uitgevoerd in aanwezigheid van een thermisch en
elektrisch geleidende metalen micro-insert die onjuist is geplaatst
(met bv. perforatie van de eileider of het myometrium als gevolg).
Alsdit zich voordoet, kan er hitte worden weggeleid van het beoogde
behandelingsgebied naar andere weefselsen/of organen die contact
maken met het geleidende voorwerp, wat voldoende kan zijn om
plaatselijk verbrandingsletsel te veroorzaken. Daarom moet worden
gecontroleerd of de metalen micro-insert op de juiste manier is
geplaatst voordat de NovaSure procedure wordt uitgevoerd.
Technisch
• Gebruik de steriele eenmalige disposable werkset niet wanneer
de verpakking beschadigd lijkt te zijn of anderszins tekenen van
onbevoegde aanraking vertoont.
• De disposable werkset is slechts voor eenmalig gebruik bestemd.
Gebruik of steriliseer de disposable werkset niet opnieuw. Het risico
van hergebruik van de disposable werkset omvat onder andere het
volgende:
• ineffectieve procedure
• infectie (ernstig)
• elektrische schok
• overdracht van besmettelijke ziekte
• scheuring van de cervix
• uterusperforatie
• Indien onmiddellijk voor een behandeling met het NovaSure systeem
een hysteroscopieprocedure met hypotonische vloeistof is uitgevoerd,
moet de uterusholte voor aanvang van de NovaSure behandeling met
normale fysiologisch-zoutoplossing worden gespoeld. De aanwezigheid
van hypotonische vloeistof kan de werkzaamheid van het NovaSure
systeem verminderen.
• Het aansluiten van de disposable werkset op de regelaar start het
uitdrijven van lucht uit de disposable werkset en de slangen door de
CO2-doorstroming. Deze priming duurt ongeveer 10seconden en moet

5
NEDERLANDS
worden uitgevoerd terwijl de disposable werkset zich nog buiten
het lichaam van de patiënt bevindt, om het risico van gas- of
luchtembolie uit te sluiten. Er wordt een bericht Apparaat ontluchten
weergegeven op het model 10 RFC en er klinkt een hoorbare pulstoon
tijdens de ontluchtingsprocedure. Wanneer het geluidssignaal ophoudt
en de LED niet meer knippert/het schermbericht verdwijnt, kan de
disposable werkset veilig worden ingebracht.
• Bij patiënten die een hartpacemaker of andere actieve implantaten
dragen, kunnen risico's bestaan als gevolg van interferentie met
de werking van de pacemaker, waardoor de pacemaker schade
kan oplopen. Raadpleeg de fabrikant van de pacemaker voor meer
informatie wanneer bij patiënten met een pacemaker toepassing van
het NovaSure systeem wordt beoogd.
• Ga zorgvuldig te werk om ervoor te zorgen dat de patiënt niet in
contact komt met metalen delen die geaard zijn of die over een
aanzienlijke capaciteit ten opzichte van aarde beschikken.
• Gevaar: explosiegevaar. Gebruik dit hulpmiddel niet in de nabijheid
van brandbare anesthesiemengsels. Gebruik het niet in de nabijheid
van brandbare gassen of vloeistoffen.
• Storing van de NovaSureRF-regelaar kan resulteren in onbedoelde
toename van het outputvermogen.
Voorzorgsmaatregelen
• In de vakliteratuur is gemeld dat patiënten met ernstige anteversie,
retroflexie of laterale migratie van de uterus een verhoogde kans lopen
op uteruswandperforatie tijdens intra-uteriene manipulatie.
• Tijdens procedures waarbij de uterus endochirurgisch wordt
behandeld, kan het voorkomen dat een hulpmiddel in een verkeerd
doorgangskanaal wordt ingebracht, vooral wanneer er sprake is van
ernstige anteversie, retroflexie of laterale migratie van de uterus.
Betracht voorzichtigheid om zeker te stellen dat de werkset op de
juiste wijze in de uterusholte wordt gepositioneerd.
• Het NovaSure systeem bestaat uit de volgende componenten:
- NovaSure disposable werkset voor eenmalig gebruik, met
verbindingskabel
- NovaSure RF-regelaar
- NovaSure CO2-canister
- NovaSure ontvochtiger
- NovaSure voetpedaal
- Netsnoer
Om een goede werking te waarborgen mogen nooit andersoortige
onderdelen met het NovaSure systeem worden gebruikt. Controleer de
onderdelen regelmatig op beschadigingen en gebruik ze niet wanneer
er sprake is van beschadiging. Het gebruik van andere dan de in deze
gebruiksaanwijzing vermelde kabels of accessoires kan resulteren in
verhoogde emissies of verminderde immuniteit van de RF-regelaar.
• De RF-regelaar moet in overeenstemming met de richtlijnen in
deze aanwijzingen worden geïnstalleerd en in werking gesteld,
om de elektromagnetische compatibiliteit te waarborgen. Zie tabel
Elektromagnetische emissie en immuniteit in paragraaf 'Specificaties'.
• De RF-regelaar mag niet in de nabijheid van of gestapeld met andere
apparatuur worden gebruikt. Als gestapeld gebruik of gebruik in de
nabijheid nodig is, moet de RF-regelaar worden geobserveerd, om
normale werking te waarborgen in de configuratie waarin de regelaar
wordt gebruikt.
• Draagbare en mobiele RF-communicatieapparatuur kan de RF-regelaar
beïnvloeden. Zie tabel Elektromagnetische emissie en immuniteit in
paragraaf 'Specificaties' voor aanbevolen scheidingsafstanden.
• Bij patiënten die endometriumablatie hebben ondergaan en later met
hormoonvervangende therapie worden behandeld, moet progestine
deel van de medicatie uitmaken, ter vermijding van het verhoogde
risico van endometriaal adenocarcinoom dat gepaard gaat met
oestrogeenvervangingstherapie zonder tegenbehandeling.
• De veiligheid en werkzaamheid van het NovaSure systeem is niet
volledig geëvalueerd bij de volgende categorieën patiënten:
- patiënten met een uterussondemeting groter dan 10cm
- patiënten met submucosale fibroïden die de uterusholte vervormen
- patiënten met een uterus bicornis, uterus septus of uterus subseptus
- patiënten die een medische (bv. GnRH-agonist) of chirurgische
voorbehandeling ondergaan
- patiënten die al eerder endometriumablatie hebben ondergaan
(metinbegrip van de NovaSure endometriumablatieprocedure)
- postmenopauzale patiënten
• Doe geen pogingen de regelaar te repareren als u een defect vermoedt.
Bel de Technische dienst van Hologic of een verkoopvertegenwoordiger
van Hologic voor aanwijzingen.
• De kabels naar de disposable werkset moeten zodanig worden
gepositioneerd dat contact met de patiënt of met andere draden
wordtvermeden.
• De gebruiker moet de disposable werkset op beschadigingen inspecteren
alvorens hem in gebruik te nemen.
• De afzuigslangontvochtiger is niet steriel en de verpakking mag daarom
niet in de steriele zone worden geplaatst.
• Raadpleeg het gedeelte Problemen oplossen onder ARRAY
POSITIONERINGSALARM als er een ARRAY-positioneringsbericht
wordt weergegeven op het scherm van het model 10.
• Gebruik de NovaSure afzuigslangontvochtiger niet wanneer het
dehydratiemateriaal roze van kleur is.
• De disposable werkset moet zich buiten het lichaam van de patiënt
bevinden wanneer de kabel op de daarvoor bestemde poort op het
voorpaneel van de regelaar wordt aangesloten (stap 2.15).
• De kooldioxidecanister bevat gas onder hoge druk. Als er sprake
is van een breuk in de CO2-canister of -slang, laat dan al het gas
uit de canister ontsnappen en laat de canister en/of slangen op
kamertemperatuur komen alvorens deze te hanteren.
• Vanaf het moment dat de disposable werkset op de regelaar
wordt aangesloten, is er een constante doorstroming van CO2,
totdat het CIA-gedeelte van de procedure is voltooid. Om de duur

6
NEDERLANDS
van de doorstroming van CO2 en het potentiële risico van embolie
te voorkomen, moet de plaatsingsprocedure onmiddellijk na het
inbrengen van de disposable werkset worden uitgevoerd en moet
direct daarna de CIA-test worden uitgevoerd.
• Door elektrisch geleidende voorwerpen (bv. controle-elektroden
van andere apparaten) die rechtstreeks met de elektrodeset van de
disposable werkset in aanraking komen of zich dicht daarbij bevinden,
kan elektriciteit aan de elektrodeset worden onttrokken. Dit kan de
oorzaak zijn van plaatselijk verbrandingsletsel van de patiënt of de arts,
of van verstoring van het elektrische veld van de elektrodeset. Daardoor
zou het therapeutische effect van de elektrodeset veranderen (onder- of
overbehandeling). Ook kan het leiden tot verstoring van de elektriciteit in
het geleidende object: er kunnen bv. onjuiste uitlezingen op de monitors
verschijnen.
• Betrouwbare aarding kan alleen worden gerealiseerd wanneer de
apparatuur is aangesloten op een voedingsaansluiting die speciaal
geschikt is voor ziekenhuisgebruik.
• Ter voorkoming van risico voor de patiënt en de gebruikers mag deze
apparatuur niet worden gebruikt in aanwezigheid van intentioneel
magnetische, ultrasone of hittebronnen.
• De cervicale ring moet volledig in zijn proximale positie ingetrokken zijn
om schade aan de schacht te vermijden wanneer de set wordt gesloten.
• De NovaSure werkset is gecontra-indiceerd voor gebruik bij vrouwen die
zwanger zijn of dat in de toekomst nog willen worden. Zwangerschap na
ablatie kan zowel voor de moeder als voor de foetus gevaarlijk zijn. Een
degelijke medische beoordeling is geboden.
Klinische gegevens inzake NovaSure over een 3-jarige
periode
Ongewenste voorvallen
Het NovaSure systeem is geëvalueerd tijdens een gerandomiseerd,
prospectief, multi-center klinisch onderzoek van 265patiënten met
abnormale uterusbloeding. In dit onderzoek werd het NovaSure
systeem vergeleken met een controlegroep die werd behandeld met
draadlusresectie van het endometrium gevolgd door rollerball-ablatie.
Tabel 1A. Intraoperatieve ongewenste voorvallen
Ongewenst voorval
NovaSure
n=175 (%)
Lusresectie plus
rollerball
n=90 (%)
Bradycardie 1 (0,6%) 0 (0,0%)
Uterusperforatie 0 (0,0% 3 (3,3%)
Cervixruptuur 0 (0,0% 2 (2,2%)
Cervixstenose 0 (0,0% 1 (1,1%)
TOTAAL 1 (0,6%) 6 (6,7%)
Tabel 1B. Postoperatieve ongewenste voorvallen <24 uur
Ongewenst voorval
NovaSure
n=175 (%)
Lusresectie plus
rollerball
n=90 (%)
Bekkenpijn/krampen 6 (3,4%) 4 (4,4%)
Misselijkheid en/of braken 3 (1,7%) 1 (1,1%)
TOTAAL 9 (5,1%)* 5 (5,6%)**
* Negen voorvallen gemeld, bij 6 (3,4%) patiënten
** Vijf voorvallen gemeld, bij 4 (4,4%) patiënten
Tabel 1C. Postoperatieve ongewenste voorvallen >24 uur – 2 weken
Ongewenst voorval
NovaSure
n=175 (%)
Lusresectie plus
rollerball
n=90 (%)
Hematometra 1 (0,6%) 0 (0,0%
Urineweginfectie 1 (0,6%) 1 (1,1%)
Vaginale infectie 1 (0,6%) 0 (0,0%
Endometritis 0 (0,0% 2 (2,2%)
Inflammatoire bekkenaandoening 0 (0,0% 1 (1,1%)
Hemorragie 0 (0,0% 1 (1,1%)
Bekkenpijn/krampen 1 (0,6%) 1 (1,1%)
Misselijkheid en/of braken 1 (0,6%) 1 (1,1%)
TOTAAL 5 (2,9%)* 7 (7,8%)**
* Vijf voorvallen gemeld, bij 4 (2,3%) patiënten
** Zeven voorvallen gemeld, bij 6 (6,7%) patiënten

7
NEDERLANDS
Tabel 1D. Postoperatieve ongewenste voorvallen >2 weken – 1 jaar
Ongewenst voorval
NovaSure
n=175 (%)
Lusresectie plus
rollerball
n=90 (%)
Hysterectomie 3 (1,7%) 2 (2,2%)
Hematometra 1 (0,6%) 2 (2,2%)
Urineweginfectie 2 (1,1%) 2 (2,2%)
Vaginale infectie 5 (2,9%) 2 (2,2%)
Endometritis 2 (1,1%) 1 (1,1%)
Inflammatoire bekkenaandoening 2 (1,1%) 0 (0,0%
Hemorragie 1 (0,6%) 0 (0,0%
Bekkenpijn/krampen 5 (2,9%) 6 (6,7%)
TOTAAL 21 (12,0%)* 15 (16,17%)**
* 21 voorvallen bij 19 (10,9%) patiënten
** 15 voorvallen bij 15 (16,7%) patiënten
Mogelijke postprocedurele complicaties
Bij endometriumablatieprocedures worden onder meer de volgende
postoperatieve complicaties regelmatig gemeld:
• Kramp/bekkenpijn binnen 24uur na de procedure is gemeld bij 3,4%
van de NovaSure patiënten en 4,4% van de met draadlusresectie plus
rollerball behandelde patiënten. Postoperatieve kramp kan uiteenlopen
van licht tot ernstig. Deze kramp duurt doorgaans enkele uren en
zelden langer dan de eerste dag na de procedure.
• Misselijkheid en braken binnen 24uur na de procedure is gemeld bij
1,7% van de NovaSure patiënten en 1,1% van de met draadlusresectie
plus rollerball behandelde patiënten. Wanneer zich misselijkheid en
braken voordoen, gebeurt dit doorgaans onmiddellijk na de procedure,
in samenhang met anesthesie. De klachten kunnen medicamenteus
worden behandeld.
• Vaginale uitscheiding
• Vaginale bloeding/bloederige uitscheiding
Andere ongewenste voorvallen
Net als bij alle endometriumablatieprocedures het geval is, kan er sprake
zijn van ernstig letsel of overlijden.
De onderstaande ongewenste voorvallen kunnen zich voordoen of zijn
gemeld in samenhang met het gebruik van het NovaSure systeem:
• post-ablatie tubair sterilisatiesyndroom
• met zwangerschap gerelateerde complicaties (opmerking:
zwangerschap na endometriumablatie is zeer gevaarlijk voor
zowel de moeder als de foetus.)
• verbrandingsletsel van omliggend weefsel
• perforatie van de uteruswand
• moeite met defecatie of mictie
• uterusnecrose
• lucht- of gasembolie
• infectie of sepsis
• complicaties met ernstig letsel of overlijden als gevolg
Klinisch onderzoek
Doelstelling: De veiligheid en doeltreffendheid van toepassing van
het NovaSure systeem werd vergeleken met draadlusresectie van
het endometrium gevolgd door rollerball-ablatie, bij premenopauzale
vrouwen die leden aan menorragie als gevolg van benigne oorzaken.
Voorbehandeling: Patiënten die in de NovaSure groep waren
gerandomiseerd, ontvingen geen endometriale voorbehandeling
(bv.hormoonbehandeling, dilatatie en curettage (D&C) of timingcontrole).
Patiënten die naar de controlegroep waren gerandomiseerd, werden als
endometriale voorbehandeling met draadlusresectie behandeld.
Eindpunten van het onderzoek: De primaire effectiviteitsmaatstaf was
een gevalideerd menstruatiedagboek-scoringssysteem dat is ontwikkeld
door Higham (Higham JM, O'Brien PMS, Shaw RW Br J Obstet Gynaecol
1990; 97:734-9). Het bloedverlies door menstruatie werd bepaald met
behulp van een 'Pictorial Blood Loss Assessment Chart' (PBLAC; grafisch
bloedverliesbepalingsoverzicht). Als slagingsfactor voor de patiënten gold
een vermindering van de menstruele vloed 1jaar na de procedure, volgens
een dagboekscore van <75. Als slagingsfactor voor het onderzoek gold
een statistisch verschil kleiner dan 20% in slagingsscores van de patiënten
tussen het NovaSure endometriumablatiesysteem met impedantieregeling
en draadlusresectie gevolgd door rollerball-ablatie. Na 2en3jaar werd er
met de patiënten contact opgenomen, met een serie vragen over het verloop
van hun bloedingen in de voorliggende 12maanden. Na 2en3jaar werd de
status van menstruele bloeding van de individuele patiënten bepaald met
gebruikmaking van de PBLAC-score over 1 jaar en het bloedingspatroon
als referentie. Daardoor was het mogelijk het bloedingspatroon of de
menstruele status van een patiënt bij 1jaar postoperatief rechtstreeks te
vergelijken met het bloedingspatroon bij 2en3jaar.
Secundaire eindpunten waren onder meer de anesthesiebehandeling, de
duur van de procedure en de antwoorden op een enquête over de kwaliteit
van leven. De veiligheidsbeoordeling werd gebaseerd op de tijdens het
onderzoek gemelde ongewenste voorvallen.
Methoden: In 9klinische centra is een gerandomiseerd (2:1)
prospectief klinisch onderzoek uitgevoerd, waaraan 265met menorragie
gediagnosticeerde patiënten deelnamen. De menstruatiedagboekscores
werden preoperatief eenmalig en postprocedureel maandelijks gedurende
12maanden verzameld. De patiënten werden op willekeurige momenten
tijdens hun menstruele cyclus behandeld. Geen van de patiënten werd
vooraf hormonaal behandeld om het endometrium te laten slinken.
Bijde tot de controlegroep behorende patiënten werd als mechanische
endometriumvoorbehandeling hysteroscopische draadlusresectie
van het endometrium uitgevoerd, gevolgd door rollerball-ablatie.
Deonderzoekdeelnemers moesten aan de volgende hoofdselectiecriteria
voldoen:
Inclusiecriteria
• Refractaire menorragie zonder definieerbare organische oorzaak
(disfunctionele uterusbloeding)
• Leeftijd tussen 25 en 50jaar
• Uterussondemeting 6,0–10,0cm (ostium externum tot inwendige fundus)

8
NEDERLANDS
• PBLAC-score van minimaal >150 gedurende 3maanden voorafgaand
aan deelname aan het onderzoek, of PBLAC-score van >150 gedurende
1maand voor vrouwen:
- die gedurende ten minste 3 voorafgaande maanden (aantoonbaar)
mislukte medische behandeling hadden ondergaan
- met een contra-indicatie tegen medische behandeling
- die medische behandeling weigerden.
Exclusiecriteria
• Patiënt lijdt aan bacteriëmie, sepsis of een andere actieve systemische
infectie
• Actieve of recidiverende chronische inflammatoire bekkenaandoening
• Patiënten die een gedocumenteerde coagulopathie hebben of
antistollingsmiddelen gebruiken
• Symptomatische endometriose
• In het verleden uitgevoerde uteruschirurgie (met uitzondering van
sectio caesarea vaginalis) waardoor de integriteit van de uteruswand is
verstoord, bv. transmurale myomectomie of klassieke sectio caesarea
• In het verleden uitgevoerde endometriumablatie
• Patiënt gebruikt geneesmiddelen waardoor het myometrium kan slinken,
zoals langdurig gebruik van steroïden
• Wens van de patiënt om nog kinderen te krijgen of om de vruchtbaarheid
te behouden
• Patiënt maakt gebruik van hormonale geboortebeperking of is niet bereid
om na de ablatie niet-hormonale geboortebeperking toe te passen
• Abnormale/ondoorgankelijke holte, waargenomen middels
hysteroscopie, saline-infusion sonografie (SIS) of hysterosalpinogram
(HSG). Meer specifiek:
- Uterus septus of uterus bicornis, of andersoortige congenitale
misvormingen van de uterusholte
- Leiomyomen met steeltje, submuceuze leiomyomen of andere
leiomyomen die de holte verstoren; poliepen (groter dan 2cm) die
mogelijk de oorzaak zijn van de menorragie van de patiënt
- De aanwezigheid van een intra-uterien anticonceptivum
• Vermoeden van of histologisch vastgestelde maligniteit van de uterus
in de voorgaande 5 jaar
• Histologisch aangetoonde endometriumhyperplasie
• Onbehandelde cervixdysplasie
• Verhoogde spiegels follikelstimulerend hormoon (FSH), duidend op
ovariumfalen >40IE/ml
• Zwangerschap
• Een actieve seksueel overdraagbare ziekte
Patiëntenpopulatie: In totaal namen 265patiënten deel aan dit
onderzoek. De leeftijd van de patiënten lag tussen 25 en 50 jaar,
waarbij 46% jonger dan 40 en 54% 40jaar of ouder was. Tussen de
behandelgroepen, de leeftijdsgroepen en de 9 onderzoekcentra waren
er geen verschillen in demografische parameters of gynaecologische
voorgeschiedenis.
Tabel 2. Patiëntenverantwoording
Aantal patiënten NovaSure Draadlusresectie
plus rollerball
Ingeschreven voor deelname
(Intent-to-treat populatie) 175 90
Afgebroken procedures*1-4 -2
Behandeld 171 88
Aanvullende behandeling* -4 -2
Hysterectomie*2-3 -2
Follow-up verzuimd of gestaakt* -5 -2
Ziekte van Hodgkin* -1 0
Bekkenpijn - leuprolide toegediend* -1 0
Beschikbare gegevens na 12 maanden
follow-up 157 82
Aanvullende behandeling* -2 -1
Hysterectomie*2-3 -1
Follow-up verzuimd of gestaakt* -2 -5
Overgeslagen bezoek -1 -1
Deelname geweigerd* -1 0
Zwangerschap* -1 0
Beschikbare gegevens na 24 maanden
follow-up 147 74
Aanvullende behandeling* 0 -4
Hysterectomie*2-5 -1
Follow-up verzuimd of gestaakt* -4 -2
Follow-up na 36maanden 138 67
Follow-up na 24 maanden verzuimd,
hervat na 36maanden
+1 +1
Beschikbare gegevens na 36maanden
follow-up 139 68
* Patiënten bij wie de deelname is beëindigd
1 Vier NovaSure-patiënten voldeden niet aan inclusiecriteria volgens protocol; twee rollerball-patiënten hadden
uterusperforatie
2 Voor hysterectomie, zie tabel 7
Resultaten
Primair effectiviteitseindpunt: bloedingsscore
Als slagingsfactor voor patiënten 12 maanden na de procedure
geldt een vermindering van de dagboekscore van >150 preoperatief
tot <75postprocedureel. Voor amenorroe geldt een score van 0.
Als slagingsfactor na 24 en 36maanden geldt verdwijnen van de
bloedingen of vermindering tot licht of normaal bloedverlies, bepaald
door telefonische enquête. De gegevens in tabel 3 (hieronder) stellen de
klinische resultaten voor, gebaseerd op het totale aantal van 265 voor
het onderzoek gerandomiseerde patiënten (intent-to-treat-groep [ITT-
groep]). Hier wordt het worst-case-scenario weergegeven, waarin ieder
van de patiënten bij wie deelname is beëindigd (in tabel 2 beschreven
onder Patiëntenverantwoording) als 'mislukt' wordt beschouwd bij het
berekenen van de waarden in de tabel.

9
NEDERLANDS
Tabel 3. Effectiviteit: Slagingscijfers – Intent-to-treat-patiënten
NovaSure
(n=175)
Draadlusresectie
plus rollerball
(n=90)
Maanden na ablatie 12* 24** 36** 12* 24** 36**
Aantal geslaagde
patiënten 136 143 134 67 68 63
Slagingscijfers onderzoek
77,7% 81,7% 76,6% 74,4% 75,6% 70,0%
Aantal patiënten met
amenorroe 63 64 58 29 26 23
Frequentie van
amenorroe
36,0% 36,6% 33,1% 32,2% 28,9% 25,6%
* Gebaseerd op dagboekscores
** Gebaseerd op telefonische enquête
Secundair effectiviteitseindpunt: kwaliteit van leven
De kwaliteit van leven van de patiënt (QOL; Quality of Life) werd bepaald
door middel van de vragenlijst Kwaliteit van leven (SF-12) en de vragenlijst
Invloed menstruatie, voor aanvang van de behandeling en 3, 6, 12, 24 en
36maanden na de procedure. In tabel4 staat de respons van de patiënten
van beide groepen, preoperatief (voor zover van toepassing) en 12, 24 en
36maanden postprocedureel.
Tabel 4. Effectiviteit: levenskwaliteit (QOL)
NovaSure Draadlusresectie
plus rollerball
Aantal patiënten dat reageerde op de vragenlijst Kwaliteit van leven#
Preoperatief 175 90
12 maanden 154 82
24 maanden 143 73
36 maanden 139 67
Percentage patiënten dat 'Tevreden' of 'Zeer tevreden' antwoordde
12 maanden 92,8% 93,9%
24 maanden 93,9% 89,1%
36 maanden 96,3% 89,7%
Percentage patiënten dat deze procedure waarschijnlijk of beslist aan
anderen zou adviseren
12 maanden 96,7% 95,9%
24 maanden 96,6% 94,5%
36 maanden 97,8% 92,6%
Aantal patiënten met dysmenorroe
Preoperatief 57,1% 55,6%
12 maanden 20,8%& 34,2%*,&
24 maanden 20,3%* 30,1%*
36 maanden 17,3%* 28,4%*
Aantal patiënten met premenstrueel syndroom (PMS)
Preoperatief 65,1% 66,7%
12 maanden 36,4%* 35,4%*
24 maanden 44,0%* 46,6%*
36 maanden 34,5%* 41,2%*
Tabel 4. Effectiviteit: levenskwaliteit (QOL)
NovaSure Draadlusresectie
plus rollerball
Percentage patiënten dat meldde soms, regelmatig of altijd door de
menstruatie moeite te hebben met het uitvoeren van werk of andere
activiteiten
Preoperatief 66,3% 65,5%
12 maanden 9,9%* 8,6%*
24 maanden 14,5%* 15,0%*
36 maanden 16,3%* 13,3%*
Percentage patiënten dat meldde zich soms, regelmatig of altijd zorgen
te maken vanwege de menstruatie
Preoperatief 74,7% 68,9%
12 maanden 23,6%* 18,5%*
24 maanden 24,2%* 19,2%*
36 maanden 18,7%* 19,1%*
Percentage patiënten dat meldde soms, regelmatig of altijd sociale
activiteiten mis te lopen vanwege de menstruatie
Preoperatief 63,3% 62,2%
12 maanden 8,5%* 8,6%*
24 maanden 9,0%* 11,1%*
36 maanden 8,1%* 10,8%*
# De vragenlijst is niet door alle patiënten ingevuld
* Statistisch significant verschil met preoperatieve respons (chi-kwadraat; p<0,05)
& Statistisch significant verschil tussen de NovaSure-groep en de rollerball-groep (chi-kwadraat; p=0,02)
Veiligheidseindpunt
Gegevens over ongewenste voorvallen zijn te vinden in paragraaf
'Ongewenste voorvallen' van deze handleiding.
Secundair eindpunt: duur van de procedure
De duur van de procedure, een secundair eindpunt, werd bij alle individuele
patiënten bepaald door het vastleggen van het tijdstip van plaatsing van het
hulpmiddel en het tijdstip van verwijdering. De gemiddelde behandelingsduur
was bij de NovaSure-patiënten aanmerkelijk korter dan bij de rollerball-groep
(respectievelijk 4,2 ± 3,5 minuten en 24,2 ± 11,4 minuten). De gemiddelde
duur van blootstelling aan RF-energie was bij een subgroep van gemonitorde
NovaSure-patiënten 84,0 ± 25,0 seconden (tabel5).
Tabel 5. Duur van de operatieprocedure
Operatieparameters NovaSure
n=175
Draadlusresectie
plus rollerball
n=90
Aantal behandelde patiënten* 171 88
Behandelingsduur in minuten
(± standaarddeviatie)
(vanaf inbrengen tot uitnemen
van het hulpmiddel)
4,2 ± 3,5** 24,2 ± 11,4**
Behandelingsduur in seconden
(± standaarddeviatie)
(duur van energieafgifte)
84,0 ± 25,0 NB#

10
NEDERLANDS
* Zie tabel 2 voor patiëntenverantwoording
** Statistisch significant verschil tussen de behandelgroepen (Student's t-test; p<0,05)
# Niet bepaald
Secundair eindpunt: anesthesiebehandeling
De keuze van anesthesiemethoden werd overgelaten aan de patiënt,
de klinisch onderzoeker en de behandelend anesthesioloog. Onder de
NovaSure-patiënten werd de procedure bij 27,0% (47/174) uitgevoerd
onder algehele of epidurale anesthesie en bij 73,0% (127/174) onder
plaatselijke en/of INTRAVENEUZE verdoving. Bij 1 patiënt in deze groep is
geen melding gemaakt van de gekozen anesthesiebehandeling. Van de
rollerball-groep werd 82,2% (74/90) van de patiënten onder algehele of
epidurale anesthesie behandeld, en 17,8% (16/90) onder plaatselijke en/
of INTRAVENEUZE verdoving (tabel6).
Tabel 6. Anesthesiebehandeling
NovaSure
n=175*
Draadlusresectie
plus rollerball
n=90
Algeheel of epiduraal 27,0% 82,2%
Plaatselijke en/of intraveneuze verdoving 73,0% 17,8%
* Bij één patiënt is geen melding gemaakt van de gekozen anesthesiebehandeling.
Klinische waarnemingen
Hysterectomie
Bij 15 vrouwen werd binnen 3 jaar na de behandeling hysterectomie
uitgevoerd. In tabel7 zijn de redenen voor hysterectomie vermeld.
Tabel 7. Hysterectomie
Reden voor hysterectomie NovaSure
n=175
Draadlusresectie
plus rollerball
n=90
Diagnose van adenocarcinoom bij
ablatieprocedure 1 1
Fibroïden 2 0
Bekkenabces 1 1
Endometriose 3 0
Adenomyose 4 0
Hematometra 0 1
Menorragie 0 1
TOTAAL 11 (6,3%) 4 (4,4%)
Bij patiënten van <40jaar is 7 maal hysterectomie uitgevoerd (7 NovaSure) en bij patiënten van >40jaar
8maal (4 NovaSure; 4 rollerball).
Patiënten selecteren
Menorragie kan door uiteenlopende onderliggende problemen worden
veroorzaakt, onder meer endometriumkanker, myomen, poliepen,
geneesmiddelen en disfunctionele uterusbloeding (anovulatoire
bloeding). De patiënten moeten altijd voor aanvang van ongeacht welke
behandeling worden gescreend en beoordeeld ter vaststelling van
de oorzaak van overmatige uterusbloeding. Raadpleeg alvorens een
endometriumablatieprocedure uit te voeren medische literatuur over de
verschillende endometriumablatietechnieken, indicaties, contra-indicaties,
complicaties en risico's.
Patiënten begeleiden
Zoals bij alle procedures wenselijk is, moet de arts alvorens
endometriumablatie uit te voeren de risico's, de voordelen en
alternatieve behandelingen met de patiënt bespreken. De verwachtingen
van de patiënt moeten zodanig worden bijgesteld dat de patiënt begrijpt
dat de behandeling als doel heeft het verminderen van de bloeding tot
een normaal niveau.
De disposable werkset is alleen bedoeld voor vrouwen zonder
zwangerschapswens, aangezien de kans op zwangerschap na de
procedure aanzienlijk zal zijn verminderd. Patiënten in de vruchtbare leeftijd
moeten worden geattendeerd op de complicaties die zich bij een eventuele
zwangerschap kunnen voordoen. In dit advies moet (indien relevant) ook
denoodzaak van postprocedurele anticonceptie worden meegenomen.
Deze procedure is geen sterilisatieprocedure en eventuele zwangerschap
na de behandeling kan voor moeder en foetus gevaarlijk zijn.
Tijdens de eerste paar weken na ablatie treedt doorgaans vaginale
afscheiding op. Deze klachten kunnen wel een maand aanhouden.
Over het algemeen wordt de afscheiding tijdens de eerste paar dagen
als bloederig beschreven. Na ongeveer 1 week wordt de afscheiding
serosanguinolent, en daarna overvloedig en waterig. Als er sprake is van
ongewone of onaangenaam ruikende afscheiding, moet dit onmiddellijk
aan de arts worden gemeld. Andere veel voorkomende postprocedurele
complicaties zijn kramp/bekkenpijn, misselijkheid en braken.
Andere veel voorkomende postprocedurele complicaties zijn kramp/
bekkenpijn, misselijkheid en braken. Indien patiënten postoperatief klagen
over acute buikpijn, koorts, kortademigheid, duizeligheid, hypotensie of
andere symptomen die kunnen samenhangen met uterusperforatie met of
zonder beschadiging van aangrenzende organen in de buikholte, moet in
de differentiële diagnose rekening worden gehouden met uterusperforatie.
De patiënten moet worden geadviseerd dergelijke symptomen onmiddellijk
aan hun arts te melden.
Voorbehandeling van de patiënt
Met het NovaSure endometriumablatiesysteem met impedantieregeling
worden met succes uterusholtebehandelingen verricht bij uiteenlopende
endometriumdiktes. Voorafgaand aan de procedure hoeven geen
maatregelen te worden genomen om de binnenste bekledende laag van
de uterus te doen slinken en de procedure kan tijdens de proliferatieve
of de secretoire fase van de cyclus worden uitgevoerd. Hoewel de
veiligheid en de effectiviteit van het NovaSure systeem nog niet volledig
zijn beoordeeld bij patiënten die een medicamenteuze of chirurgische
voorbehandeling hebben ondergaan, is een dergelijke beoordeling wel
uitgevoerd bij een beperkt aantal patiënten die waren voorbehandeld
met GnRH-agonisten zonder dat daarbij complicaties of ongewenste
voorvallen waren opgetreden.
Vastgesteld is dat actieve bloeding geen beperkende factor vormt voor het
gebruik van het NovaSure systeem. Geadviseerd wordt ten minste 1 uur
voor de behandeling een niet-steroïde anti-inflammatoir geneesmiddel
(NSAID) toe te dienen en deze medicatie postoperatief voort te zetten, om
de kans op intraoperatieve en postoperatieve uteruskrampen te verkleinen.

11
NEDERLANDS
Gebruiksaanwijzing NovaSure endometriumablatiesysteem
met impedantieregeling
Lees alle instructies, voorzorgsmaatregelen en waarschuwingen alvorens
het product te gebruiken.
1.0 Opstellen
NovaSure
RF-REGELAAR
NovaSure DISPOSABLE WERKSET
MET VERBINDINGSKABEL, INCLUSIEF
AFZUIGSLANGONTVOCHTIGER
NovaSure NETSNOER NOVASURE AFZUIGSLANG-
ONTVOCHTIGER
NovaSure CO2-CANISTER NOVASURE VOETPEDAAL
1.1 Bij het werken met het NovaSure systeem zijn de volgende
componenten nodig:
• 1 steriele NovaSure disposable werkset voor eenmalig gebruik, met
• verbindingskabel
• 1 NovaSure RF-regelaar
• 1 NovaSure voetpedaal
• 1 NovaSure wisselstroomnetsnoer
• 1 NovaSure niet-steriele afzuigslangontvochtiger
• 1 NovaSure CO2-canister
Vacuüm-
ontluchtingsklep
Cervicale ring
Tweepolige
elektrode-set
Voorste greep
Schacht
Achterste
greep
Afzuig-
slang
Ontgrendelingsknop
Holtelengte-instelling
Vacuüm-
retourslang
met geribbelde
aansluiting
'WIDTH'-
meetschijf
Opmerking: Zorg dat er ten minste 1 extra disposable werkset,
ontvochtiger en CO2-canister voorhanden zijn.
1.2 Prepareer de NovaSure RF-regelaar. Plaats de regelaar op een
tafeltje naast de patiënt, binnen het gezichtsveld van de chirurg.
Sluit het wisselstroomnetsnoer aan op de regelaar en op een
wisselstroomcontactdoos.
1.3 Schroef de CO2-canister stevig vast in de regelaar op de achterzijde
van de regelaar.
Tuimel-
schakelaar
CO2-canister
Netsnoer
1.4 Draai de CO2-regelknop geheel naar de HI-stand (indien hiermee
uitgerust).
Opmerking: Regelaars van nieuwere modellen zijn niet uitgerust
met een regelknop; de doorstroming van CO2 wordt daarin
automatisch geregeld. Ga verder naar stap 1.5 indien uw regelaar
niet met een regelknop is uitgerust.
1.5 Druk de tuimelschakelaar op het achterpaneel van de regelaar in
deaan-stand.
1.6 Sluit het voetpedaal aan op de juiste poort op het voorpaneel van
deregelaar.
Opmerking: Wanneer RF-regelaar model 10 voor het eerst
wordt ingeschakeld, verschijnt het scherm 'Selecteer uw taal'.
Destandaardinstelling is Engels. Om een andere taal te selecteren
drukt u op de knop met de naam van de beoogde taal. Sla de
selectie op door op de groen knipperende knop te drukken.
De geselecteerde taal blijft behouden. Via het scherm 'Instellingen'
kunt u de aanvankelijk ingestelde taalselectie desgewenst wijzigen.
Druk op de naam van de taal om de op het scherm gebruikte taal te
wijzigen. Om de wijzigingen van de instellingen op te slaan, drukt u
op de groen knipperende knop. Om een selectie te annuleren drukt
u op de blauwe 'X'.
2.0 Procedure
2.1 Prepareer de patiënt voor anesthesie.
Poort

12
NEDERLANDS
2.2 Leg de patiënt in steensnedeligging.
2.3 Voer anesthesie uit volgens de standaard.
2.4 Voer met beide handen lichamelijk onderzoek uit. Beoordeel of er
sprake is van ernstige anteversie of retroversie.
2.5 Prepareer de patiënt en dek haar af, op dezelfde wijze als bij een
dilatatie- en curettageprocedure.
2.6 Breng een speculum in de vagina in.
2.7 Houd met een tenaculum de cervix vast.
2.8 Voer een sondemeting van de uterus uit, vanaf de fundus tot het
ostium externum uteri. De doelmatigheid van het NovaSure
systeem is nog niet volledig geëvalueerd bij patiënten met
eenuterussondemeting groter dan 10cm.
2.9 Bepaal de lengte van het cervixkanaal en dilateer het kanaal
voor plaatsing van de werkset.
OPMERKING: De diameter van de NovaSure disposable werkset
bedraagt nominaal 6mm.
2.10 Neem de uterussondemeting en de cervixkanaalmetingen als
uitgangspunt om de juiste holtelengte-instellingen te bepalen in de
tabel Holtelengte (hieronder). Boven in de tabel vindt u aangepaste
afmetingen die de elektrodelengtes van de disposable werkset
weergeven.
Een juiste bepaling van de holtelengte is belangrijk voor een veilige
en effectieve behandeling. Wanneer de holtelengte wordt overschat,
kan dit leiden tot verbrandingsletsel van het endocervicale kanaal.
Waarschuwing: Ga bij sonderen, dilateren en bij het inbrengen
van de disposable werkset voorzichtig te werk om perforatie van
deuteruswand te voorkomen.
TABEL 8. HOLTELENGTE
Uterussonde (cm)
Cervixlengte
(cm) 10 9,5 9 8,5 8 7,5 7 6,5 6
26,5* 6,5* 6,5* 6,5 6 5,5 5 4,5 4
2,5 6,5* 6,5* 6,5 6 5,5 5 4,5 4
36,5* 6,5 6 5,5 5 4,5 4
3,5 6,5 6 5,5 5 4,5 4
46 5,5 5 4,5 4
4,5 5,5 5 4,5 4
55 4,5 4
5,5 4,5 4
64
* De waarde 6,5 is geen weerspiegeling van het numerieke verschil tussen de sondelengte en de lengte van
het cervixkanaal.
De waarde 6,5 is toegevoegd, omdat dit de maximale lengte vertegenwoordigt die de NovaSure set kan
bereiken.
Contra-indicatie: Behandel een patiënt niet wanneer de lengte van
de uterusholte minder dan 4cm is, aangezien dit beschadiging van
het cervixkanaal kan veroorzaken.
Opmerking: Bij patiënten met een uterusholtelengte van meer
dan 6,0cm werden lagere slagingspercentages gemeten dan het
slagingspercentage van het totale onderzoek.
2.11 Open de steriele verpakking van de NovaSuredisposable werkset.
Leg de disposable werkset met verbindingskabel in de steriele
zone. Ga hierbij voorzichtig te werk en zorg dat de doos met de
niet-steriele afzuigslangontvochtiger buiten de steriele zone blijft.
Waarschuwing: Gebruik de steriele, voor eenmalig gebruik
bestemde disposable werkset niet wanneer de verpakking
beschadigd lijkt te zijn of anderszins tekenen van onbevoegde
aanraking vertoont.
2.12 Open de doos en het zakje van de niet-steriele afzuigslangontvochtiger.
Verwijder de rode doppen.
Let op: De afzuigslangontvochtiger is niet steriel en de verpakking
mag daarom niet in de steriele zone worden geplaatst.
Let op: Indien de afzuigslangontvochtiger roze is gekleurd, moet
deze voor aanvang van de ablatieprocedure worden vervangen.
2.13 Sluit de ontvochtiger aan op de geribbelde aansluiting van de
afzuigslang van de disposable werkset. Zorg dat de geribbelde
aansluiting volledig in de slang van de ontvochtiger wordt ingebracht.
2.14 Let op: De disposable werkset moet uitwendig (buiten) de patiënt
zijn gepositioneerd totdat stap 2.15 kan worden uitgevoerd.
2.15 Sluit de kabel van de disposable werkset aan op de juiste poort op
het voorpaneel van de regelaar.
Disposable werkset Poort

13
NEDERLANDS
Waarschuwing: Het aansluiten van de NovaSure disposable werkset
op de NovaSureRF-regelaar start het uitdrijven van lucht uit de
disposable werkset en de slangen door de CO2-doorstroming. Deze
priming duurt ongeveer 10seconden en moet worden uitgevoerd
terwijl de disposable werkset zich nog buiten het lichaam van
de patiënt bevindt. Er wordt een bericht Apparaat ontluchten
weergegeven op het model 10 RFC en er klinkt een hoorbare pulstoon
tijdens de ontluchtingsprocedure. Wanneer het geluidssignaal
ophoudt en de LED niet meer knippert/het schermbericht verdwijnt,
kan de NovaSure disposable werkset veilig worden ingebracht.
Let op: Vanaf het moment dat de disposable werkset op de regelaar
wordt aangesloten is er een constante doorstroming van CO2,
totdat het CIA-gedeelte van de procedure is voltooid. Om de duur
van de doorstroming van CO2 en het potentiële risico van embolie
te voorkomen, moet de plaatsingsprocedure onmiddellijk na het
inbrengen van de disposable werkset worden uitgevoerd en moet
direct daarna de CIA-test worden uitgevoerd.
Waarschuwing: Ga bij sonderen, dilateren en bij het inbrengen
van de disposable werkset voorzichtig te werk om perforatie van
deuteruswand te voorkomen.
2.16 Activeer het wegwerpapparaat buiten de patiënt en zorg ervoor dat
het schermbericht niet op de Model 10 RFC wordt weergegeven
wanneer de array wordt geopend. Als het schermbericht nog
steeds wordt weergegeven op het model 10 RFC, moet u het
wegwerpapparaat sluiten en opnieuw openen. Als het probleem
hiermee niet is opgelost, moet de disposable werkset worden
vervangen.
2.17 Verzeker u ervan dat de 'WIDTH'-meetschijf een waarde van 4,0cm
of meer aangeeft.
'WIDTH'-
meetschijf
Opmerking: Wanneer de 'WIDTH'-meetschijf minder dan 4,0cm
aangeeft, sluit dan de disposable werkset en herhaal de hierboven
beschreven stap 2.16. Geeft de 'WIDTH'-meetschijf nog steeds
een wijdte van minder dan 4,0cm aan, open dan een nieuwe
disposable werkset en retourneer de oude disposable werkset aan
de technische ondersteuning van Hologic.
2.18 Ontgrendel de disposable werkset door op de ontgrendelingsknop
te drukken. Sluit de disposable werkset door de voorste greep stil
te houden en de achterste greep naar achteren te trekken, totdat op
de 'Closed Array'-indicator, die zich op de scharnier van de voorste
en achterste greep bevindt, 'ARRAY CLOSED' (set gesloten) wordt
weergegeven. Dit duidt erop dat de set in de schacht is ingetrokken
en de disposable werkset zich in gesloten positie bevindt.
'ARRAY
CLOSED'-
indicator
Ontgrendelingsknop
2.19 Controleer of de elektrodeset volledig door de externe schacht
wordt omsloten.
2.20 Controleer of de 'WIDTH'-meetschijf circa 0,5cm aangeeft.
2.21 Neem de uterussondemeting en de cervixkanaalmetingen als
uitgangspunt om de juiste holtelengte-instellingen te bepalen in de
tabel Holtelengte (hierboven), zoals eerder omschreven in stap 2.10.
Contra-indicatie: Behandel een patiënt niet wanneer de lengte van
de uterusholte minder dan 4cm is, aangezien dit beschadiging van
het cervixkanaal kan veroorzaken.
2.22 Selecteer aan de hand van de tabel Holtelengte in paragraaf 2.10
de waarde voor de lengte in het invoerscherm van de NovaSure
RF-regelaar met behulp van de pijltoetsen.
2.23 Stel de holtelengte-instelling van de disposable werkset in op de
eerder verkregen waarde en vergrendel deze instelling. (Ziestap2.21.)
Controleer of de cervicale ring volledig is ingetrokken in de proximale
positie.
2.24 Controleer of de cervix daadwerkelijk is gedilateerd tot minimaal
6mm (de nominale diameter van de NovaSure disposable werkset).
2.25 Houd enige spanning op het tenaculum om de hoek van de uterus
zo klein mogelijk te houden.
2.26 Houd de disposable werkset onder een zodanige hoek dat deze in
lijn is met de as van de uterus tijdens het transcervicaal inbrengen
van de disposable werkset in de uterusholte. Voer de disposable
werkset op door de voorste greep stil te houden, totdat het distale
uiteinde van de schacht de fundus raakt.

14
NEDERLANDS
#10
Waarschuwing: Als de disposable werkset moeilijk in het
cervixkanaal kan worden ingebracht, moet op grond van klinisch
inzicht worden bepaald of verdere dilatatie gewenst is.
2.27 Trek de disposable werkset circa 0,5 cm van de fundus terug.
Drukde handgrepen langzaam samen (NIET VERGRENDELEN)
totdatde weerstand toeneemt.
De 'WIDTH'-meetschijf moet ongeveer 0,5cm aangeven. Op dit
punt is de externe schacht ingetrokken.
0,5 cm
2.28 Blijf de handgrepen van de disposable werkset langzaam
samendrukken en beweeg ondertussen de disposable werkset
~0,5cm naar de fundus toe en van de fundus af, waarbij de
handgreep van de disposable werkset 45° linksom ten opzichte van
het verticale vlak en 45° rechtsom ten opzichte van het verticale
vlak wordt rondgedraaid totdat de handgrepen vergrendelen.
De 'WIDTH'-meetschijf moet een waarde aangeven van meer dan
2,5cm.
Opmerking: Zodra de handgrepen van de disposable werkset
zijn vergrendeld, moet de uterus met de disposable werkset
meebewegen.
2.29 Beweeg de disposable werkset voorzichtig voorwaarts, achterwaarts
en zijwaarts.
2.30 De plaatsing wordt voltooid door de disposable werkset iets terugte
trekken totdat de 'WIDTH'-meetschijf afneemt met circa 0,2–0,5cm.

15
NEDERLANDS
Opmerking: een juiste plaatsing van de elektrodeset tegen de fundus is belangrijk voor een veilige en effectieve behandeling. Als een deel
van de elektrodeset of de distale rand van de externe schacht tijdens de behandeling in het endocervicale kanaal is geplaatst, is er een
verhoogd risico op verbrandingsletsel van het endocervicale kanaal.
Fundus
Elektrodeset
Rand van de schacht
Endocervicaal kanaal
Rand van de schacht bevindt zich
in onderste segment van uterus
Elektrodeset
Endocervicaal kanaal Rand van de schacht
Rand van de schacht bevindt
zich in endocervicaal kanaal
Fundus
ONJUISTE PLAATSING JUISTE PLAATSING
2.31 Houd het tenaculum vast en voer de disposable werkset langzaam
en voorzichtig op tot de fundus. De ‘WIDTH’-meetschijf moet een
waarde aangeven hoger dan of gelijk aan de vorige.
2.32 Schuif de cervicale ring naar voren door matige druk op de lip
op de cervicale ring uit te oefenen, totdat de cervicale ring een
afdichting vormt tegen het ostium externum uteri.
2.33 Lees de cornu-tot-cornu-afstand (minimaal 2,5cm) op de 'WIDTH'-
meetschijf.
Lichte druk
Stevige druk
Contra-indicatie: Behandel een patiënt niet wanneer de breedte
van de uterusholte minder dan 2,5cm is, bij meting met de ‘WIDTH’-
meetschijf van de disposable werkset nadat de werkset is geplaatst.
Let op: Als de ‘ARRAY POSITION’-mededeling verschijnt: raadpleeg
paragraaf ‘Problemen oplossen’, alinea ‘ARRAY POSITION-alarm’.
2.34 Selecteer de waarde zoals aangegeven op de ‘WIDTH’-meetschijf in
het invoerscherm van de NovaSure RF-regelaar met behulp van de
pijltoetsen.
2.35 Het systeem kan bestuurd worden in de automatische of
handmatige modus. In automatische modus start de ablatiecyclus
automatisch na een geslaagde ‘Cavity Integrity Assessment’ (CIA).
In handmatige modus start de ablatiecyclus niet automatisch na
een geslaagde CIA.

16
NEDERLANDS
Besturing van RF-regelaar model 10
A. Automatische modus
Voor automatische besturing van RF-regelaar model 10 drukt u op
de knop 'Switch-modus' wanneer deze onder aan het scherm
verschijnt. Ga verder met stap 2.36, maar volg stap 2.37 niet als
het systeem automatisch wordt bestuurd.
B. Handmatige modus
Opmerking: De handmatige modus is de standaard
besturingsmodus van het systeem.
Voor handmatige besturing van het systeem drukt u niet op de knop
'Switch-modus' voor aanvang van de CIA ('Cavity Integrity
Assessment'). Volg stap 2.36 en 2.37.
2.36 Start de CIA-procedure door het voetpedaal eenmaal in te drukken.
Op het scherm wordt 'Holtemeting wordt uitgevoerd' weergegeven
terwijl vijf puntjes opeenvolgend oplichten en uitgaan. De test duurt
ongeveer 7 tot 30seconden. Het scherm 'Holtemeting voltooid'
verschijnt wanneer de CIA is voltooid en het systeem RF-energie
kan afgeven. Er kan geen energie aan de disposable werkset
worden afgegeven totdat het scherm 'Holtemeting voltooid' wordt
weergegeven.
Als de 'Cavity Integrity Assessment' mislukt, verschijnt het scherm
'Holtemeting mislukt' met probleemoplossingsstappen.
A. Bij vermoeden van perforatie moet de procedure onmiddellijk
worden beëindigd.
B. Als de CIA-test opnieuw mislukt, moet u controleren of er lekkages
in het systeem en tussen de cervix en de cervicale ring bestaan.
Controleer alle slangaansluitingen en verzeker u ervan dat een
afzuigslangontvochtiger is geïnstalleerd. Als er lekkage blijkt te
zijn bij de cervix welke niet met de cervicale ring kan worden
verholpen, gebruikt u een ander tenaculum om de cervix rond de
schacht vast te pakken. Herhaal de CIA-test door het voetpedaal in
te drukken.
Opmerking: Bij het ostium externum uteri kan zich CO2-lekkage
voordoen als gevolg van een overgedilateerde cervix. Onder
dergelijke omstandigheden kan een CO2-lekkage gepaard gaan met
zichtbare luchtbellen of een 'sissend' geluid van ontsnappend gas.
C. Wanneer de 'Cavity Integrity Assessment' na redelijke pogingen om
de probleemoplossingsprocedures (stap 2.36) te implementeren
geen resultaat oplevert, moet de procedure worden stopgezet.
Opmerking: Als de disposable werkset na het uitvoeren van een
'Cavity Integrity Assessment' uit de uterusholte is verwijderd, moet
als de disposable werkset weer wordt ingebracht voorafgaand aan
een ablatie opnieuw een CIA-test worden uitgevoerd (ongeacht of
de CIA eerder was geslaagd).
2.37 Alleen voor de handmatige modus
Tijdens handmatige besturing van het systeem start de ablatiecyclus
niet automatisch na een geslaagde 'Cavity Integrity Assessment'.
Naeen geslaagde CIA, druk op de toets 'ENABLE' en druk nogmaals
op het voetpedaal om de ablatiecyclus te starten.
Opmerking: Bij alle RF-regelaars model 10 vindt automatisch
een voortest vacuümsubsysteem plaats voor aanvang van de
ablatiecyclus. Het scherm 'Vacuümcontrole wordt uitgevoerd'
verschijnt en er klinkt gedurende 10 seconden een piepsignaal
tijdens de voorcontrole van het vacuümsubsysteem.
Tijdens de ablatiecyclus verschijnt het scherm 'RF AAN' met een
timer om de duur van de ablatie bij te houden.
Opmerking: De RF-energieafgifte kan op elk gewenst moment
worden stopgezet door indrukken van het voetpedaal.
2.38 Na automatische beëindiging van de ablatiecyclus (circa
90seconden) trekt u de cervicale ring volledig in zijn proximale
positie in met behulp van de lip op de cervicale ring.
Let Op: De cervicale ring moet volledig in zijn proximale positie
ingetrokken zijn om schade aan de schacht te vermijden wanneer
de set wordt gesloten.
Cervicale
ring

17
NEDERLANDS
Bij voltooiing van de ablatiecyclus verschijnt het scherm 'Procedure
voltooid' met een samenvatting van de procedure. In het scherm 'Procedure
voltooid' wordt de volgende informatie van elke procedure vastgelegd:
• Uteruslengte
• Uterusbreedte
• Vermogensinstelling
• RF-ablatietijd
2.39 Ontgrendel de disposable werkset door op de ontgrendelingsknop
te drukken. Sluit de disposable werkset door de voorste greep stil te
houden en de achterste greep voorzichtig naar achteren te trekken,
totdat op de 'Closed Array'-indicator, die zich op de scharnier van de
voorste en achterste greep bevindt, 'ARRAY CLOSED' (set gesloten)
wordt weergegeven. Dit duidt erop dat de set in de schacht is
ingetrokken en de disposable werkset zich in gesloten positie bevindt.
Opmerking: Als het moeilijk is de disposable werkset te sluiten en
verwijderen, raadpleeg dan paragraaf 'Problemen oplossen', alinea
'Moeilijkheden bij sluiten en verwijderen van de disposable werkset
post-ablatie'.
Let Op: Ga bij het terugtrekken van de set voorzichtig te werk om
schade aan het hulpmiddel te voorkomen.
2.40 Verwijder de disposable werkset uit de patiënt.
2.41 SCHAKEL DE NOVASURE RF-REGELAAR UIT.
2.42 Verleen postoperatieve zorg aan de patiënt volgens de
standaardprocedures.
2.43 Ontsla de patiënt uit het ziekenhuis of de kliniek volgens voorschrift
van de behandelend arts.
Periodiek onderhoud en service
De RF-regelaar is ontworpen en getest om te voldoen aan IEC 60601-
1 en andere veiligheidsnormen. Onderhoud is niet nodig, omdat het
systeem zelfcontroles uitvoert wanneer de stroom wordt ingeschakeld.
Voor reiniging van de regelaar raadpleegt u de sectie “Reinigen en
ontsmetten
De verwachte levensduur van de RF-controller is vijf jaar of 2000
procedures, op voorwaarde dat schade door fysieke impact, zoals
vallen of ruwe hantering, wordt voorkomen. Als de controller valt of
ernstige fysieke beschadiging ondervindt, moet u het gebruik stopzetten
en contact opnemen met de technische ondersteuning van Hologic.
Raadpleeg het gedeelte Technische ondersteuning en informatie over het
retourneren van producten.
Er is voor de NovaSure RF-regelaar geen onderhoudshandleiding
beschikbaar aangezien de unit geen componenten bevat waarvoor
onderhoud noodzakelijk is.
Waarschuwing: Wijzigingen aan deze apparatuur zijn niet toegestaan.
RF-vermogensoutputtest
Bij de NovaSure RF-regelaar model 10 is het automatisch testen van de
vermogensoutput geïntegreerd in een zelftest bij aanzetten (POST -
Power On Self Test). Gedurende de POST wordt de vermogensoutput van
de regelaar (Pc) afgegeven aan een shuntweerstand (Rs-shunt resistor)
die zich in de regelaar bevindt. De Pc is ingesteld op 180W en de Rs is
nominaal 25ohm. Er wordt gedurende de POST geen stroom afgegeven aan
de connector van de disposable werkset die zich aan de voorzijde van de
regelaar bevindt.
De NovaSure RF-regelaar model 10 voert tijdens het opstarten
automatisch de POST uit. Ga voor informatie over de POST naar
Instellingen en blader naar Systeeminformatie. Druk op knop 'Tooninfo'.
Opmerking: Schakel op de netvoedingsmodule de voeding uit,
wanneer gedurende de POST een systeemstoring optreedt, en
herhaal hierna de POST. Stel de RF-regelaar buiten werking
wanneer er voor de tweede maal een systeemstoring optreedt en
neem contact op met de Technische ondersteuning van Hologic.
Let Op: Doe geen pogingen de regelaar te repareren als u een
defect vermoedt. Volg de aanwijzingen beschreven in 'Problemen
oplossen' in deze handleiding. Neem voor aan-wijzingen telefonisch
contact op met de Technische dienst van Hologic indien de
problemen aanhouden.
NovaSure steriele disposable werkset: geen onderhoud noodzakelijk.
Bestemd voor eenmalig gebruik. Gebruik of steriliseer de NovaSure
disposable werkset niet opnieuw.

18
NEDERLANDS
Schermpictogrammen NovaSure RF-regelaar model 10
Hieronder volgt een beschrijving van de pictogrammen op het scherm
van de NovaSure RF-regelaar model 10.
Pictogram Instellingen:
Druk op deze knop om de
instelopties voor taal, helderheid
en volume weer te geven.
Pictogram Laatste procedure:
Druk op deze knop om het scherm
'Procedure voltooid' weer te geven
en de samenvatting van de laatste
procedure te bekijken.
Pictogram Hulp:
Druk op deze knop om meer informatie over
de huidige procedurestap weer te geven.
Ditpictogram geeft een verkorte versie van
de taal van de gebruiksaanwijzing weer.
Opmerking: Wanneer op het pictogram 'Laatste procedure' wordt
gedrukt, wordt alleen de vorige procedure weergegeven. Informatie
over procedures voorafgaand aan de meest recente procedure is
niet beschikbaar.
Opmerking: Druk in het scherm 'Instellingen' op de knoppen '-' of
'+' om het volume en de helderheid aan te passen.
Opmerking: Wanneer de RF-regealaar model 10 voor het eerst
wordt ingeschakeld, verschijnt het scherm 'Selecteer uw taal'. De
standaardinstelling is Engels. Om een andere taal te selecteren
drukt u op de knop met de naam van de beoogde taal. Sla de
selectie op door op de groen knipperende knop te drukken. De
geselecteerde taal blijft behouden. Via het scherm 'Instellingen'
kunt u de aanvankelijk ingestelde taalselectie desgewenst wijzigen.
Druk op de naam van de taal om de op het scherm gebruikte taal te
wijzigen. Om de wijzigingen van de instellingen op te slaan, drukt u
op de groen knipperende knop. Om een selectie te annuleren, drukt
u op de blauwe 'X'.
Problemen oplossen - de meest voorkomende alarmen
'CAVITY ASSESSMENT'-ALARM
Als de 'Cavity Integrity Assessment' mislukt, verschijnt het scherm
'Holtemeting mislukt' met een verkorte versie van de onderstaande
probleemoplossingstips. De 'Cavity Integrity Assessment' (CIA) mislukt
doordat de holte niet onder druk kan worden gebracht. Mogelijke
oorzaken zijn:
1. Lekkage van de werkset: Controleer of de filter van de
afzuigslangontvochtiger is geïnstalleerd. Controleer alle
slangaansluitingen om er zeker van te zijn dat deze stevig vastzitten.
2. Lekkage bij het ostium externum uteri: Let op zichtbare luchtbellen
of een 'sissend' geluid bij het ostium externum uteri.
Gebruik de lip op de cervicale ring om de cervicale ring op te
voeren tegen het ostium externum uteri zodat er een nauwsluitende
afdichting ontstaat. Voer de CIA-test opnieuw uit. Als de CIA-test
opnieuw mislukt, gebruikt u een tweede tenaculum om de cervix
rond de schacht van de NovaSure disposable werkset vast te
pakken. Voer de CIA-test opnieuw uit.
3. Uterusperforatie: Bij vermoeden van perforatie moet de
procedure onmiddellijk worden beëindigd.
Opmerking: Bij het ostium externum uteri kan zich CO2-lekkage
voordoen als gevolg van een overgedilateerde cervix. Onder
dergelijke omstandigheden kan een CO2-lekkage gepaard gaan met
zichtbare luchtbellen of een 'sissend' geluid van ontsnappend gas.
Opmerking: Bij het uitvoeren van probleemoplossingsstappen
voor de RF-regelaar model 10 kunt u op de knop '?' op het
scherm drukken en de schuifknoppen aan de rechterzijde
gebruiken om meer informatie te krijgen. Om vanuit de extra
probleemoplossingstips terug te gaan naar het hoofdscherm,
druktu op de 'X' in de rechter bovenhoek van het scherm.
Wanneer de 'Cavity Integrity Assessment' na redelijke pogingen om
de probleemoplossingsprocedures (stap 2.36) te implementeren geen
resultaat oplevert, moet de procedure worden stopgezet.
'VACUÜM'-ALARM
Het 'vacuüm'-alarm treedt op als het vacuümniveau buiten het
gespecificeerde bereik ligt. Dit kan zich voordoen als gevolg van een
ofmeer van de volgende oorzaken:
• een overgedilateerde cervix;
• slecht contact tussen de cervicale ring en het ostium externum uteri;
• de vacuümontluchtingsklep bevindt zich in gesloten positie;
• een blokkade in de disposable werksetfilter(s) (2) of ontvochtiger; of
• een blokkade in de disposable werkset.
Als de vacuümcontrole mislukt, verschijnt het scherm 'Vacuümfout' met
een verkorte versie van de volgende probleemoplossingstips:
• Duw voorzichtig een uterusdilatator of -sonde van 2–3,5 mm in de
vacuümontluchtingsklep.
• Controleer de positie van de cervicale ring en herpositioneer deze,
indien nodig. Gebruik de lip op de cervicale ring om de cervicale

19
NEDERLANDS
ring op te voeren tegen het ostium externum uteri zodat er een
nauwsluitende afdichting ontstaat. Controleer of er geen lucht door de
cervix wordt gezogen doordat er speling is tussen de cervicale ring
en de ingang naar het cervicale kanaal. Probeer, indien er lucht in het
cervicale kanaal wordt gezogen, de cervicale ring en de schacht van
de disposable werkset te herpositioneren, zodat luchttoevoer wordt
voorkomen.
• Verzeker u ervan dat de afzuigcanister op de disposable werkset
verticaal ligt en dat de werksetslangen niet over het been van de
patiënt liggen.
• Controleer alle slangaansluitingen om er zeker van te zijn dat
deze stevig vastzitten. Controleer de slangverbindingen die op de
dehydratieslang worden gedrukt. Vervang de ontvochtiger indien deze
roze is. Verzeker u er van dat de filter, die zich dichtbij de disposable
aansluiting op de vacuümretourslang bevindt, stevig vast zit.
• Voer opnieuw een ablatie uit.
Als het scherm 'Vacuümfout' opnieuw wordt weergegeven:
• Maak de disposable werkset los van de RF-regelaar.
• Verwijder de disposable werkset en vervang deze door een nieuwe.
• Voer met de nieuwe werkset opnieuw een ablatie uit.
Opmerking: Bij het uitvoeren van de probleemoplossingsstappen
voor de RF-regelaar model 10 kunt u op de knop '?' op het
scherm drukken en de schuifknoppen aan de rechterzijde
gebruiken om meer informatie te krijgen. Om vanuit de extra
probleemoplossingstips terug te gaan naar het hoofdscherm, drukt
u op de 'X' in de rechter bovenhoek van het scherm.
Beëindig de procedure als met de nieuwe werkset het vacuümalarm
optreedt.
Opmerking: Als de disposable werkset na het uitvoeren van een
'Cavity Integrity Assessment' uit de uterusholte is verwijderd, moet
als de disposable werkset weer wordt ingebracht voorafgaand aan
een ablatie opnieuw een CIA-test worden uitgevoerd (ongeacht of
de CIA eerder was geslaagd).
CO2-canister bijna of helemaal leeg
Er verschijnt een scherm met de melding 'Vervang CO2' en een
afbeelding van de achterkant van de regelaar. Er klinkt een toon met
een frequentie van eenmaal per seconde. Alarmberichten die aanwezig
waren voordat het alarm optrad blijven aanwezig tijdens het voorval
Vervang CO2. De geluidswaarschuwing wordt niet opgeheven door het
indrukken van het voetpedaal.
1. Vervang de CO2-canister zodat het piepsignaal wordt opgeheven.
Opmerking: De disposable werkset hoeft, voorafgaand aan het
vervangen van de canister, niet uit de patiënt te worden verwijderd.
2. Vervolg de procedure.
'ARRAY POSITION'-alarm
Het 'Array Position'-bericht wordt weergegeven wanneer de elektrodeset
niet volledig geopend is. Er kan geen ablatie worden uitgevoerd met de
regelaar wanneer het 'Array Position'-bericht wordt weergegeven. Als
het 'ARRAY POSITION'-alarm optreedt, verschijnt het scherm 'Controleer
waaier' met een verkorte versie van de volgende probleemoplossingstips:
1. Verplaats het proximale uiteinde van de disposable werkset voorzichtig
en kijk of het 'Array Position'-bericht verdwijnt. Blijfthetbericht
aanwezig, dan vervolgt u de procedure als volgt:
2. Probeer de NovaSure disposable werkset voorzichtig te herpositioneren:
A. Trek de set gedeeltelijk terug in de schacht door de
ontgrendelingsknop op de handgreep van de disposable
werkset te ontgrendelen;
B. Trek de disposable werkset enigszins terug van de fundus;
C. Open de disposable werkset langzaam opnieuw, terwijl u de
disposable werkset voorzichtig voor- en achterwaarts beweegt
en de handgrepen van de disposable werkset vergrendelt; en
D. Plaats de disposable werkset opnieuw tegen de fundus volgens
de plaatsingsprocedure beschreven in de stappen 2.26 tot en
met 2.33.
3. Ga zorgvuldig te werk wanneer er sprake is van uteriene retroversie,
zodat perforatie wordt voorkomen. Voer met het tenaculum
voorzichtig caudale tractie op de cervix uit en beweeg tijdens de
plaatsingsprocedure de handgreep van de disposable werkset in de
richting van het plafond (in lijn met de as van de uterus).
4. Indien het 'Array Position'-bericht nog steeds wordt weergegeven:
trek de disposable werkset geheel terug en verwijder de set uit het
lichaam van de patiënt.
5. Ontrol de disposable werkset buiten het lichaam van de patiënt;
controleer of de elektrodeset onbeschadigd is en of het 'Array
Position'-bericht verdwijnt.
6. Ga bij het opnieuw inbrengen, opnieuw ontrollen of herpositioneren
van de disposable werkset te werk volgens deplaatsingsprocedure
beschreven in paragraaf 2.0.
7. Indien het 'Array Position'-bericht nog steeds wordt weergegeven,
moet de disposable werkset worden vervangen door een nieuwe set.
8. Indien bij gebruik van een nieuwe disposable werkset het 'Array
Position'-bericht wordt weergegeven, moet de procedure worden
afgebroken.
Opmerking
: Bij het uitvoeren van de probleemoplossingsstappen voor
de RF-regelaar model 10 kunt u op de knop '?' op het scherm drukken
en de schuifknoppen aan de rechterzijde gebruiken om meer informatie
te krijgen. Om vanuit de extra probleemoplossingstips terug te gaan
naar het hoofdscherm, drukt u op de 'X' in de rechter bovenhoek van het
scherm.
Ga naar de volgende pagina voor de rest
van de gebruiksaanwijzing. Aanvullende
probleemoplossing.

20
NEDERLANDS
Vermoeden van uterusperforatie
Voorafgaand aan het toepassen
van energie:
1. Beëindig de procedure.
2. Zorg dat de patiënt stabielligt.
3. Overweeg de behandeling van
de perforatie.
4. Plan de procedure opnieuw,
indien van toepassing.
Tijdens of na het toepassen van
energie:
1. Beëindig de procedure.
2. Zorg dat de patiënt stabielligt.
3. Sluit visceraal letsel uit.
4. Plan de procedure opnieuw,
indien van toepassing.
Set ontrolt en vergrendelt zich niet volledig in de uterus
1. Trek de set gedeeltelijk terug in de schacht (houd de voorste greep
vast en trek de achterste greep naar achteren, weg van depatiënt).
2. Herpositioneer de disposable werkset in de holte.
3. Ontrol de set opnieuw in de holte.
4. Wanneer de disposable werkset niet wordt vergrendeld, moetdeze
uit de uterus worden verwijderd.
5. Controleer de disposable werkset op beschadiging.
6. Probeer de disposable werkset te openen en te vergrendelen, buiten
het lichaam van de patiënt.
7. Wanneer de disposable werkset beschadigd is, moet deze worden
vervangen.
8. Wanneer de disposable werkset onbeschadigd is, kan de set
opnieuw in de uterusholte van de patiënt worden ingebracht en kunt
u proberen de set te openen.
9. Wanneer het niet mogelijk is de disposable werkset te openen
op een cornu-tot-cornu-afstand van minstens 2,5cm, moet de
procedure worden afgebroken.
10. Overweeg uterusperforatie als mogelijke oorzaak van het niet
ontrollen van de set.
Moeilijkheden bij sluiten en verwijderen van de disposable
werkset na ablatie
Controleer of de ontgrendelingsknop is ingedrukt:
• Indien dit het geval is, trek geleidelijk de disposable werkset uitde
patiënt.
• Indien dit niet het geval is, drukt u op de ontgrendelingsknop en
probeert u opnieuw de disposable werkset te sluiten. Indien de set nog
steeds moeilijk te sluiten is, trekt u geleidelijk de disposable werkset
uit de patiënt.
Het scherm Procedure voltooid verschijnt niet op het model 10
RFC aan het einde van een procedure.
Als de stroom ten minste 30 seconden niet aangesloten is geweest,
verschijnt het scherm Procedure voltooid niet op het model 10 RFC.
Procedure Niet voltooid
1. Verwijder het apparaat van de patiënt en plaats de array
a. Controleer of de array NIET beschadigd is
b. Controleer of de arraypositie NIET wordt weergegeven
2. Druk op ? voor meer hulp.
Als a en b zijn gecontroleerd, kunt u het apparaat opnieuw
inbrengen en DE VOETSCHAKELAAR INDRUKKEN om de
behandeling opnieuw uit te voeren.
Als er een probleem wordt geconstateerd, vervangt u het
apparaat en start u de procedure opnieuw.
1. Verwijder de NovaSure disposable werkset uit de uterus nadat de set
volledig in de schacht is teruggetrokken.
A. Ontgrendel de ontgrendelingsknop van de disposable werkset.
B. Houd de voorste greep van de disposable werkset stevig vast.
C. Trek de achterste greep van de disposable werkset naar achteren.
2. Controleer de disposable werkset op eventuele beschadigingen.
Activeer de elektrodearray volledig buiten de patiënt om aan te tonen
dat het bericht niet wordt weergegeven op het model 10 RFC .
3. Als het wegwerpapparaat niet beschadigd is en het schermbericht
niet wordt weergegeven op het model 10 RFC, moet u het opnieuw
inbrengen, opnieuw activeren en de behandeling opnieuw uitvoeren.
4. Vervang de huidige disposable werkset door een nieuwe wanneer
het probleem blijft bestaan.
5. Voer de procedure opnieuw uit. Beëindig de procedure wanneer het
probleem blijft bestaan.
Het scherm RF AAN wordt niet weergegeven op het model 10
RFC
1. Controleer het voetpedaal wanneer er vanuit de regelaar geen energie
geleverd wordt als het voetpedaal wordt ingedrukt, terwijl de NovaSure
RF-regelaar is aangesloten, is ingeschakeld en de toets 'ENABLE' is
ingedrukt. Controleer ook of de 'CAVITY ASSESSMENT' is voltooid.
2. Beëindig de procedure wanneer het probleem blijft bestaan.
UP/DOWN-waarden verschijnen niet wanneer de bijbehorende
toetsen worden ingedrukt
Controleer of de disposable werkset op de regelaar is aangesloten.
Dewaarden verschijnen alleen als de disposable werkset correct op
deregelaar is aangesloten.
Instructies voor vervanging van onderdelen
De NovaSure RF-regelaar maakt gebruik van twee zekeringen die
zich bevinden op de zekeringhouder in de netvoedingsmodule. De
zekeringen die worden gebruikt zijn van het type T5AH, 250V. Er
kan toegang worden verkregen tot de module met behulp van een
sleufschroevendraaier, waarmee u het deurtje van de zekeringhouder
openwipt. Desgewenst kan de zekeringhouder hierna worden verwijderd
en kunnen de zekeringen worden vervangen. Voor het plaatsen van
de zekeringhouder volgt u bovenstaande stappen in omgekeerde
volgorde. Een NovaSure product dat mogelijk defecten vertoont, moet
ter beoordeling aan Hologic worden geretourneerd. Volg de aanwijzingen
beschreven in paragraaf 'Retourzending voor onderhoud en reparatie'

21
NEDERLANDS
aan het einde van deze handleiding, voor het verkrijgen van een
retourmaterialenautorisatienummer (RMA-nr.: Returned Materials
Authorization number). Werp de NovaSure disposable werkset niet weg.
Technische specificaties
NovaSure disposable werkset
1. De NovaSure disposable werkset bevat geen latex.
2. De NovaSure disposable werkset is een hulpmiddel Klasse III volgens
de richtlijnen van de FDA.
3. De NovaSure disposable werkset is een hulpmiddel Klasse IIB
volgens EU-richtlijn MDD93/42/EEG
4. Nominale diameter van de NovaSure disposable werksettip: 6 mm.
5. Totale afmetingen van de NovaSure disposable werkset:
48,3cm x 15,2cm x 5cm.
6. De NovaSure disposable werkset heeft een nominaal voltage van 153 V.
NovaSure RF-regelaar
1. De NovaSure RF-regelaar kan worden gebruikt met uitgangen van
100 tot 240 VAC en trekt maximaal 5 ampère.
2. De NovaSure RF-regelaar is een Klasse I, defibrillatorbestendig,
Type BF-instrument volgens norm IEC 60601-1.
3. De NovaSure RF-regelaar is een toestel Klasse III volgens de
richtlijnen van de FDA.
4. De NovaSure RF-regelaar is een hulpmiddel Klasse IIB volgens
EU-richtlijn MDD93/42/EEG.
5. De RF-regelaar is getest en in overeenstemming bevonden met de
grenswaarden voor medische hulpmiddelen volgens IEC 60601-
1-2 ED 4.0: 2014. Deze bepalingen zijn opgesteld om te voorzien
in behoorlijke bescherming tegen gevaarlijke interferentie in een
gebruikelijke medische installatie. Deze apparatuur genereert en
gebruikt radiofrequentie-energie, en kan deze energie uitstralen. Indien
de apparatuur niet overeenkomstig de instructies wordt geïnstalleerd
en gebruikt, kan deze energie interferentie met andere instrumenten
in de omgeving veroorzaken. Er is echter geen garantie dat er bij een
bepaalde installatie geen interferentie zal optreden. Als de apparatuur
toch schadelijke interferentie veroorzaakt aan andere apparaten (wat
kan worden bepaald door de apparatuur aan en uit te zetten), wordt
de gebruiker aangeraden de interferentie te verhelpen met een van de
volgende maatregelen:
• Draai de ontvangende apparatuur of zet deze op een andere plaats
• Vergroot de afstand tussen de apparaten
• Sluit de apparatuur aan op een wandcontactdoos in een ander
circuit dan waarop de/het andere appara(a)ten zijn/is aangesloten
• Neem contact op met de Technische Dienst van Hologic (of de
fabrikant van de andere apparatuur) voor ondersteuning.
6. De regelaar voldoet aan de eisen opgenomen in IEC60601-1/
UL60601-1, IEC60601-2-2 en CSAC22.2 nr.601.1.
7. De regelaar mag uitsluitend worden verzonden in de originele
verpakking van Hologic. Omgevingsvereisten voor gebruik,
verzending en opslag vindt u hieronder.
8. De NovaSureRF-regelaar genereert een absoluut maximaal
piekvoltage van 153volt. Accessoires die met de RF-regelaar worden
gebruikt, moeten een nominaal voltage van 153 volt of hoger hebben.
9. De NovaSureRF-regelaar genereert een absoluut maximaal
piekvermogen van 216watt.
10. Gewicht van de NovaSureRF-regelaar: 11kg, onverpakt.
11. Hoogte: 32 cm; breedte: 19 cm; diepte: 35,5 cm.
12. De maximale CO2-druk, afgegeven door de NovaSure RF-regelaar en
disposable werkset, is 90 ±10mmHg. Wanneer de NovaSure RF-
regelaar is aangesloten op de disposable werkset, is de maximale
CO2-flowsnelheid 95 ±15ml/min. (Wanneer de NovaSure RF-regelaar
niet is aangesloten op de disposable werkset, is de maximale CO2-
flowsnelheid 105 - 130 ml/min.)
13. De NovaSure RF-regelaar moet worden gebruikt zonder neutrale
elektrode.
Vermogen vs. weerstand
Gemeten vermogen (watt)
Belastingweerstand (ohm)
Effectief vermogen vs. vermogensinstelling in een belasting
van 20 ohm
Effectief vermogen (watt)
Vermogensinstelling (watt)

22
NEDERLANDS
Omgevingsomstandigheden
NovaSure RF-regelaar
In bedrijf, zonder verpakking
Hoogte 0 tot 3.030 m (0 tot 10.000 voet)
Temperatuur 10 °C tot 40 °C (50 °F tot 104 °F)
Vochtigheid 15 tot 85% relatieve vochtigheid
(nietcondenserend)
Buiten bedrijf, met verpakking
Hoogte 0 tot 12.120 m (0 tot 40.000 voet)
Temperatuur -30 °C tot 60 °C (-22 °F tot 140 °F)
Vochtigheid 85% relatieve vochtigheid, (nietcondenserend)
maximaal 90% RV,( niet-condenserend)
Belangrijke prestaties Kenmerken
• Het hulpmiddel moet gedurende 10 seconden worden ontlucht
voordat het bij de patiënt wordt ingebracht.
• De Cavity Integrity Assessment (CIA) moet gedurende minimaal 3
seconden een druk van 50 ± 10 mmHg meten om geslaagd te zijn.
Anders meldt de CIA een fout. De RF-regelaar laat pas een ablatie
beginnen als de CIA geslaagd is.
• RF-vermogen: Het bereik van de RF-vermogensafgifte is 55 tot 180
(+/-20%) watt.
• Vacuümdrukbewaking: Tijdens een ablatie moet de vacuümdruk
tussen 17,78 ± 5,08 mmHg en 152,4 ± 25,4 mmHg liggen.
Als de vacuümdruk dit bereik overschrijdt, beëindigt de regelaar de
ablatie.
• Impedantiebewaking: De RF-controller beëindigt een ablatie als de
gemeten weefselimpedantie ongeveer 50 ohm bereikt.
• Timer (twee minuten): Na twee miuten RF-energieafgifte beëindigt
de regelaar de ablatie.
• Time-out (tien minuten): na afloop van de ablatie-ingreep wordt de
regelaar 10 minuten uitgeschakeld. Gedurende deze tijd kan de
regelaar geen energie afgeven.
• DC-kortsluitbeveiliging: Als de RF-regelaar kortsluiting detecteert
(d.w.z. <13+/-6ohms), wordt de ablatie beëindigd.
Elektromagnetische veiligheidsrichtlijnen
Tabel 1 - Richtlijnen en verklaring van de fabrikant –
Elektromagnetische emissie
Richtlijnen en verklaring van de fabrikant –Elektromagnetische
emissie
e NovaSure RF-regelaar is bestemd voor gebruik in de hieronder gespecificeerde
elektromagnetische omgeving. De klant of gebruiker van de NovaSure RF-regelaar
dient ervoor te zorgen dat het hulpmiddel in een dergelijke omgeving wordt gebruikt.
Emissietest Conformiteit Elektromagnetische omgeving -
Richtlijnen
RF-emissies
CISPR 11
Groep 1 De NovaSure RF-regelaar moet
elektromagnetische energie uitstralen
om de beoogde werking mogelijk te
maken. Hierdoor kan elektronische
apparatuur in de nabijheid worden
beïnvloed.
RF-emissies
CISPR 11
Klasse A De NovaSure RF-regelaar is bedoeld
voor gebruik in professionele
zorginstellingen, waaronder
ziekenhuizen en artsenpraktijken.
Waarschuwing: De EMISSIE-
eigenschappen van deze apparatuur
maken deze geschikt voor
toepassing in industriegebieden
en ziekenhuizen (CISPR 11, Klasse
A). Als deze apparatuur wordt
gebruikt in een woonomgeving
(waarvoor normaal gesproken
CISPR 11, Klasse B vereist is),
biedt het wellicht niet afdoende
bescherming aan radiofrequente
communicatiediensten. De
gebruiker dient wellicht
corrigerende maatregelen te nemen,
zoals het verplaatsen of verdraaien
van de apparatuur.
Harmonische
emissies
IEC 61000-3-2
Klasse A
Spanningsschom-
melingen/
flikkeremissies
IEC 61000-3-3
Voldoet
Waarschuwing: In sommige omstandigheden bestaat het risico van
brandwonden op andere dan de chirurgische plaats wanneer een
hoogfrequent apparaat wordt gebruikt. Huid-op-huid-contact dient
te worden vermeden, bv. door het inbrengen van een droog gaasje.
Waarschuwing: Bij alle elektrochirurgische apparatuur bestaat de
mogelijkheid van vonkoverslag (‘arcing’) en kan neuromusculaire
stimulatie optreden. Bij een juist gebruik van dit apparaat in de
uterus is het risico van spierstimulatie, met name van de hartspier,
uitermate klein.

23
NEDERLANDS
Tabel 2 - Richtlijnen en verklaring van de fabrikant –
Elektromagnetische immuniteit
Richtlijnen en verklaring van de fabrikant –
Elektromagnetische immuniteit
e NovaSure RF-regelaar is bestemd voor gebruik in de hieronder gespecificeerde
elektromagnetische omgeving. De klant of gebruiker van de NovaSure RF-regelaar
dient ervoor te zorgen dat het hulpmiddel in een dergelijke omgeving wordt gebruikt.
Immuniteitstest Testniveau
IEC 60601 Conformiteits-
niveau
Elektromagnetische
omgeving – Richtlijn
Elektrostatische
ontlading (ESD)
IEC 61000-4-2
±2 kV, ±4 kV,
±8 kV contact
±2 kV, ±4 kV,
±8 kV contact
Vloeren moeten van hout,
beton of keramische
tegels zijn vervaardigd.
Indien vloeren met
synthetisch materiaal zijn
bedekt, moet de relatieve
vochtigheid minimaal 30%
bedragen.
±2 kV, ±4 kV,
±8 kV, ±15 kV
lucht
±2 kV, ±4 kV,
±8 kV, ±15 kV
lucht
Snelle
elektrische
transiënten/
lawines
IEC 61000-4-4
±0,5 kV, ±1 kV,
±2 kV voor
voedingslei-
dingen
Herhalings-
frequentie
100 kHz
±0,5 kV, ±1 kV,
±2 kV voor
voedingslei-
dingen
Herhalings-
frequentie
100 kHz
De kwaliteit van de
netspanning dient gelijk
te zijn aan die van een
normale commerciële of
ziekenhuisomgeving.
Overspanning
IEC 61000-4-5
±0,5 kV, ±1 kV
leiding(en) naar
leiding(en)
±0,5 kV, ±1 kV
leiding(en) naar
leiding(en)
De kwaliteit van de
netspanning dient gelijk
te zijn aan die van een
normale commerciële of
ziekenhuisomgeving.
±0,5 kV,
±1 kV, ± 2 kV
leiding(en) naar
aarde
±0,5 kV,
±1 kV, ± 2 kV
leiding(en) naar
aarde
Spanningsdalin-
gen, korte
onderbrekingen
en spannings-
variaties op
voedingsinvoer-
leidingen
IEC 61000-4-11
0 % UT;
0,5 cyclus bij
0°, 45°, 90°,
135°, 180°,
225°, 270°
en 315°
0 % UT;
0,5 cyclus bij
0°, 45°, 90°,
135°, 180°,
225°, 270°
en 315°
De kwaliteit van de
netspanning dient gelijk
te zijn aan die van een
normale commerciële
of ziekenhuisomgeving.
Als de gebruiker van de
NovaSure RF-regelaar
continue werking wenst
tijdens onderbreking van
de hoofdstroomtoevoer,
wordt voeding van
de NovaSure RF-
regelaar middels
een ononderbroken
stroomtoevoer (UPS) of
een batterij aanbevolen.
0 % UT;
1 cyclus en
70 %UT;
25/30 cycli
Enkele fase:
bij 0°
0 % UT;
1 cyclus en
70 %UT;
25/30 cycli
Enkele fase:
bij 0°
0 % UT;
250 cycli
0 % UT;
250 cycli
Onder deze
omstandigheden
wordt de
RF-regelaar
uitgeschakeld
en keert deze
terug naar
standby-modus.
Netfrequentie
50/60 Hz
Magnetisch veld
IEC 61000-4-8
30 A/m
50 Hz
30 A/m
50 Hz
Magnetische velden met
stroomfrequentie dienen
een niveau te hebben dat
karakteristiek is voor een
locatie in een commerciële
of ziekenhuisomgeving.
Opmerking : UT is de wisselstroomspanning voorafgaand aan de toepassing
van het testniveau.

24
NEDERLANDS
T
abel 3 - Richtlijnen en verklaring van de fabrikant –
Elektromagnetische immuniteit
Richtlijnen en verklaring van de fabrikant – Elektromagnetische
immuniteit
e NovaSure RF-regelaar is bestemd voor gebruik in de hieronder gespecificeerde
elektromagnetische omgeving. De klant of gebruiker van de NovaSure RF-regelaar dient
ervoor te zorgen dat het hulpmiddel in een dergelijke omgeving wordt gebruikt.
Immuniteitstes Testniveau
IEC 6060 Conformiteits-
niveau
Elektromagnetische
omgeving – Richtlijn
Geleide RF
IEC 61000-4-6
3 V
0,15 MHz -
80 MHz
6 V in ISM-
en amateurradio-
banden tussen
0,15 MHz en
80 MHz
80% AM bij
1 kHz
3 V
0,15 MHz -
80 MHz
6 V in ISM-
en amateurradio-
banden tussen
0,15 MHz en
80 MHz
80% AM bij 1 kHz
Uitgestraalde RF
IEC 61000-4-3
3 V/m
80 MHz tot
2,7 GHz
80% AM bij
1 kHz
3 V/m
80 MHz tot
2,7 GHz
80% AM bij
1 kHz
Aanbevolen minimale
scheidingsafstand
Draagbare RF-
communicatieapparatuur
(waaronder
randapparatuur zoals
antennekabels en externe
antennes) mag niet
binnen een afstand van
minder dan 30 cm (12 in)
van alle onderdelen van
het NovaSure-systeem
voor endometriale ablatie
met impedantieregeling
worden gebruikt, met
inbegrip van kabels
gespecificeerd door
Hologic Inc. Dit kan
verslechterde prestaties
van deze apparatuur tot
gevolg hebben.
.
De veldsterkte van vaste RF-
zenders, bepaald door controle
van de elektromagnetische
omgeving,a moet lager zijn dan
het compliantieniveau
in elk frequentiebereik.b
Interferentie kan zich voordoen
in de nabijheid
van apparatuur die is voorzien
van het volgende symbool:
OPMERKING 1: Bij 80 MHz en 800 MHz geldt het hoogste frequentiebereik.
OPMERKING 2: Deze richtlijnen gelden mogelijk niet in alle situaties. De
elektromagnetische voortplanting wordt beïnvloed door de absorptie en de
reflectie van structuren, objecten en mensen.
a
De veldsterkte van vaste zenders zoals basisstations voor radiotelefoons (mobiel/draadloos) en portofoons, CB,
AM- en FM-uitzendingen en tv-uitzendingen kan niet nauwkeurig theoretisch worden voorspeld. Voor het bepalen
van de elektromagnetische omgeving die door vaste RF-zenders wordt gecreëerd, moet een elektromagnetische
meting ter plaatse worden overwogen. Als de gemeten veldsterkte op de locatie waar de RF-generator wordt
gebruikt het RF-conformiteitsniveau hierboven overschrijdt, moet worden gecontroleerd of de RF-generator naar
behoren functioneert. Wanneer de RF-generator afwijkend presteert, zijn aanvullende maatregelen nodig, zoals
het anders richten of verplaatsen van de RF-generator.
b
Binnen het frequentiebereik van 150 kHz tot 80 MHz moet de veldsterkte kleiner zijn dan 3 V/m.
Aanbevolen scheidingsafstanden tussen draagbare en mobiele
RF-communicatieapparatuur en de NovaSure
RF-regelaar
Draagbare RF-communicatieapparatuur (waaronder randapparatuur
zoals antennekabels en externe antennes) mag niet binnen een afstand
van minder dan 30 cm (12 in) van alle onderdelen van het NovaSure-
systeem voor endometriale ablatie met impedantieregeling worden
gebruikt, met inbegrip van kabels gespecificeerd door Hologic Inc. Dit
kan verslechterde prestaties van deze apparatuur tot gevolg hebben.
Reinigen en desinfecteren
Voor reiniging en desinfectie wordt het gebruik van niet-brandbare
reinigingsmiddelen aanbevolen. Brandbare middelen of oplosmiddelen
die worden gebruikt voor reiniging en desinfectie, moeten voor gebruik
van het NovaSure systeem kunnen verdampen.
De NovaSure RF-regelaar is niet steriel. Alleen de oppervlakken mogen
met een oplossing van water en een niet-agressief schoonmaakmiddel
worden afgenomen. Dompel de unit niet onder in vloeistof en laat geen
vloeistof in de koelventilatoren of bij de RF-kabels terechtkomen.
De NovaSure steriele disposable werkset is bestemd voor eenmalig
gebruik.
• Gebruik de disposable werkset niet wanneer de verpakking al eerder
geopend is geweest of beschadigd is.
• Gebruik of steriliseer de disposable werkset niet opnieuw.
Steriliseer geen onderdelen van het NovaSure
endometriumablatiesysteem met impedantieregeling.
Onderdelenlijst
Bestelinformatie, gerelateerde onderdelen en accessoires
Productnummer Beschrijving
RFC2010 NovaSure RF-regelaar model 10
814002 Netsnoer, 115 volt, Noord-Amerika
814003 Netsnoer, 230 volt, Europa
814004 Netsnoer, 220 volt, Verenigd Koninkrijk/Ierland
814005 Netsnoer, Denemarken
814009 Netsnoer, Italië
814011 Netsnoer, Zwitserland
814015 Netsnoer, Japan

25
NEDERLANDS
814016 Netsnoer, Australië
52124-001 Voetpedaal
815012 CO2 (USP), cilinder, 5-stuksverpakking
NS2013 NovaSure endometriumablatiesysteem met
impedantieregeling, disposable werksetkit
300001 Verpakking voor biologisch gevaarlijk materiaal
Afvoer
Let Op:
De gebruikte disposable werkset moet behandeld
worden als biologisch gevaarlijk afval en als zodanig worden
afgevoerd, volgens de standaardprocedures van het.
Hologic en haar distributeurs en klanten in de Europese Unie zijn verplicht
te voldoen aan de richtlijn inzake Afval van elektrische en elektronische
apparaten (AEEA) (2002/96/EG). Hologic streeft ernaar te voldoen aan
landspecifieke voorschriften met betrekking tot milieutechnisch correcte
behandeling van haar producten. Hologic stelt zich tot doel om het afval
dat voortkomt uit het afdanken van haar elektrische en elektronische
apparatuur, te verminderen. Hologic beseft de voordelen van het zo
mogelijk onderwerpen van dergelijke AEEA-apparatuur aan hergebruik,
bewerking, recycling of herwinning, om de uitstoot van gevaarlijke stoffen
in het milieu te minimaliseren. Klanten van Hologic in de Europese Unie
zijn verantwoordelijk om ervoor te zorgen dat medische apparatuur met
het hieronder afgebeelde symbool, dat aangeeft dat de AEEA-richtlijn van
toepassing is, niet in het gemeentelijke afvalsysteem worden afgevoerd,
tenzij de bevoegde instanties in uw vestigingsgebied daartoe toestemming
hebben gegeven.
Neem contact op met de technische ondersteuning van Hologic voor
afspraken voor het op de juiste wijze afvoeren van de RF-regelaar
overeenkomstig de AEEA-richtlijn.
Garantie
Tenzij uitdrukkelijk anders vermeld in de overeenkomst geldt het volgende:
i) voor de originele klant geldt dat de door Hologic geproduceerde
apparatuur gegarandeerd wezenlijk naar behoren zal werken
overeenkomstig de gepubliceerde productspecificaties voor een periode
van één (1) jaar vanaf de verzenddatum, of, indien installatie vereist is,
vanaf de installatiedatum (“Garantieperiode”); ii) röntgenbuizen voor
digitale mammografie worden gedekt door een garantie van vierentwintig
(24) maanden, tijdens welke periode de röntgenbuizen een volledige
garantie hebben voor de eerste twaalf (12) maanden en gedurende
maand 13 tot en met 24 een garantie die volgens een rechte lijn afneemt
tot nul; iii) vervangingsonderdelen en gereviseerde artikelen worden
gedekt door een garantie gedurende de resterende garantieperiode of
negentig (90) dagen vanaf verzending, waarbij de langste van de twee
geldt; iv) verbruiksgoederen voldoen gegarandeerd aan de gepubliceerde
specificaties voor een periode die afloopt op de op de respectieve
verpakkingen aangegeven vervaldatum; v) gelicentieerde software werkt
gegarandeerd overeenkomstig de gepubliceerde specificaties; vi) de
levering van diensten geschiedt gegarandeerd op professionele wijze; vii)
de garantie voor apparatuur die niet door Hologic geproduceerd is, wordt
verstrekt door de desbetreffende fabrikant en dergelijke garanties gelden
voor klanten van Hologic voor zover toegestaan door de fabrikant van
dergelijke niet door Hologic geproduceerde apparatuur. Hologic garandeert
niet dat producten zonder onderbreking of fouten zal werken, of dat
producten zullen functioneren met producten van andere fabrikanten die
niet door Hologic zijn goedgekeurd.
Deze garanties gelden niet voor artikelen die: (a) gerepareerd, verplaatst of
gewijzigd zijn door anderen dan door servicepersoneel dat geautoriseerd
is door Hologic; (b) onderhevig zijn geweest aan fysiek misbruik (inclusief
thermisch of elektrisch), spanning of verkeerd gebruik; (c) opgeslagen,
onderhouden of gebruikt zijn op een wijze die onverenigbaar is met de van
toepassing zijnde specificaties of instructies van Hologic, waaronder de
weigering van de klant om door Hologic aanbevolen software-upgrades
toe te staan; of (d) zijn aangemerkt als geleverd onder een garantie die niet
door Hologic wordt geboden of op een pre-release- of op ‘as-is’-basis.
Technische ondersteuning en informatie over
productretournering
Waarschuwing: De garantie vervalt wanneer de RF-regelaar is
gevallen, hetgeen de regelaar zodanig kan beschadigen dat reparatie
onmogelijk is. We adviseren het gebruik van een stabiele trolley
waarop de regelaar met banden kan worden bevestigd, waarmee
het risico van vallen wordt verminderd. Ga bij het verplaatsen van de
RF-regelaar naar een locatie buiten de instelling voorzichtig te werk.
Neem bij vragen met betrekking tot de RF-regelaar telefonisch
contact op met +1-800-442-9892 of +1-508-263-2900.
Servicevertegenwoordigers
Neem contact op met de Afdeling Technische ondersteuning van Hologic
voor instructies en een retourmaterialenautorisatienummer (RMA-nr.:
Return Materials Authorization number) indien de NovaSure RF-regelaar
onbruikbaar wordt. Reinig en verpak de regelaar volgens de aanwijzingen
en verzend de regelaar ter reparatie of service naar de hieronder vermelde
geautoriseerde locaties. Indien de regelaar niet onder garantie valt, zal er
na ontvangst en beoordeling van de NovaSure RF-regelaar een gepaste
vergoeding voor verwerking en reparatie worden vastgesteld.
Neem voor service, technische ondersteuning of nabestellingen in de
Verenigde Staten contact op met:

26
NEDERLANDS
Voor meer informatie
Neem voor technische ondersteuning of nabestellingen in de Verenigde
Staten contact op met:
Hologic, Inc.
250 Campus Drive
Marlborough, MA 01752 USA
Tel.: 800-442-9892 (gratis, alleen binnen de VS)
www.hologic.com
Opmerking: Voorvallen of problemen waarvan de gebruiker meent
dat deze een veiligheidsrisico kunnen vormen, dienen aan de
Afdeling Technische ondersteuning van Hologic te worden gemeld.
Internationale klanten wordt gevraagd contact op te nemen met hun
distributeur of lokale verkoopvertegenwoordiger van Hologic:
Hologic BV
Da Vincilaan 5
1930 Zaventem
Belgium
Tel: +32 2 711 46 80
Fax: +32 2 725 20 87
Rapporteer klachten of problemen met betrekking tot de kwaliteit,
betrouwbaarheid, veiligheid of prestaties van dit product aan Hologic. Als
het apparaat letsel bij de patiënt heeft veroorzaakt of verergerd, moet u
het incident onmiddellijk aan een geautoriseerde vertegenwoordiger van
Hologic en aan de bevoegde autoriteit van de respectievelijke lidstaat of
het betreffende land rapporteren. De bevoegde autoriteit voor medische
apparaten is meestal het ministerie van Gezondheid van de individuele
lidstaat of een instantie binnen het ministerie van Gezondheid.
Retourzending voor onderhoud en reparatie
Lees deze instructies voorafgaand aan het retourneren van
gebruikte/niet gebruikte, mogelijk defecte producten aan Hologic.
Neem contact op met de technische ondersteuning van Hologic als de
NovaSure disposable werkset of RF-regelaar niet overeenkomstig de
beschrijving werkt. Indien het product om bepaalde redenen aan Hologic
wordt geretourneerd, ontvangt u van de Afdeling Technische ondersteuning
een retourmaterialenautorisatienummer (RMA-nr.: Returned Materials
Authorization number) en, indien van toepassing, een verpakking voor
biologisch gevaarlijk materiaal.
Retourneer RF-regelaars volgens de instructies van de technische
ondersteuning. Reinig de RF-regelaar voordat u deze retourneert en
verpak alle accessoires samen met de geretourneerde unit in de doos.
Retourneer gebruikte of geopende disposable werksets overeenkomstig
de instructies die bij de verpakking voor biologisch gevaarlijk van Hologic
is geleverd.
Verklaring van symbolen
Symbool Norm-referen-
tie en sym-
bool-nummer
Titel van sym-
bool Beschrijving van symbool
EC R
EP
EN ISO 15223-
1, 5.1.2
Gemachtigde
vertegen-woor-
diger in de
Europese Ge-
meenschap
Geeft de gemachtigde ver-
tegenwoordiger in de Euro-
pese Gemeenschap aan.
IEC 60601-1,
Tabel D.1, 1
IEC 60417,
5032
Wisselstroom
(AC)
Geeft op het typeplaatje
aan dat de apparatuur
alleen geschikt is voor wis-
selstroom; identificeert de
relevante aansluitingen.
EN ISO 15223-
1, 5.3.9
ISO 7000, 2621
Atmos-ferische
drukgrens
Geeft de atmosferische
druk aan waaraan het
apparaat veilig kan worden
blootgesteld.
EN ISO 15223-
1, 5.1.5
ISO 7000, 2492
Lotnummer
Geeft de batchcode van
de fabrikant aan zodat de
batch of het lot kan worden
geïdentificeerd.
CO2NA Kooldioxide Geeft koolstofdioxide aan.
EN ISO 15223-
1, 5.1.6
ISO 7000, 2493
Catalogus-num-
mer
Geeft het catalogusnum-
mer van de fabrikant
aan zodat het medische
hulpmiddel kan worden
geïdentificeerd.
N/A Categorie
Niet-AP-appa-
ratuur
Identificeert de categorie
niet-AP-apparatuur.
EN ISO 15223-
1, 5.4.4
ISO 7000,
0434A
IEC 60601-1,
Tabel D.1, 10
Let op
Geeft aan dat er voor-
zichtigheid moet worden
betracht bij gebruik van
het hulpmiddel of dat het
hulpmiddel dichtbij de
locatie van symbool moet
worden gebruikt. Het geeft
tevens aan dat in de huidi-
ge situatie aandacht van de
bediener of een actie van
de bediener vereist is om
onnodige consequenties te
voorkomen.
Europese me-
dische richtlijn
93/42/EEG,
Artikel 17 en
Bijlage XII
Europese
richtlijn betref-
fende medische
hulpmiddelen
2017/745, Bij-
lage V
CE-merk voor
conformiteit
met identifica-
tie-nummer van
aangemelde
instantie
Geeft aan dat het medische
hulpmiddel aan de Euro-
pese richtlijn betreffende
medische hulpmiddelen
93/42/EEG en de van
toepassing zijnde gezond-
heids-, veiligheids- en om-
gevingsvereisten voldoet.
Als er een nummer bij de
markering wordt vermeld,
is naleving door de aange-
geven aangemelde instan-
tie geverifieerd.

27
NEDERLANDS
Symbool Norm-referen-
tie en sym-
bool-nummer
Titel van sym-
bool Beschrijving van symbool
EN ISO 15223-
1, 5.4.3
ISO 7000, 1641
IEC 60601-1,
Tabel D.1, 11
Raadpleeg de
gebruiksaan-
wijzing
Geeft aan dat de gebruiker
de gebruiksaanwijzing
moet raadplegen.
CC
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 6049
Land van fab-
ricage
Identificeert het land
waarin de producten zijn
vervaardigd
IEC 60601-1,
Tabel D.1, 24
IEC 60417,
5036
Gevaarlijk volt-
age
Geeft gevaren als gevolg
van gevaarlijke spanningen
aan
EN ISO 15223-
1, 5.1.3
ISO 7000, 2497
Productiedatum Geeft de datum aan waar-
op het medische apparaat
is geproduceerd.
IEC 60601-1,
Tabel D.1, 26
IEC 60417,
5334
Defibrillator-Defibrillator-
bestendige Type bestendige Type
BF-apparatuurBF-apparatuur
Identificeert een defibril-Identificeert een defibril-
latiebestendig toegepast latiebestendig toegepast
onderdeel van type BF onderdeel van type BF
conform IEC 60601-1.conform IEC 60601-1.
EN ISO 15223-
1, 5.2.6
ISO 7000, 2608
Niet hersterili-
seren
Geeft aan dat de onder-
delen die met de patiënt
in aanraking komen geen
ftalaten bevatten.
EN ISO 15223-
1, 5.4.2
ISO 7000, 1051
IEC 60601-1,
Tabel D.1, 28
Niet hergebrui-
ken
Geeft een medisch hulp-
middel aan dat bestemd is
voor eenmalig gebruik.
ISO 7000, 2403
ISO 780
Niet hoger sta-
pelen dan ‘n’
Geeft aan dat de items niet
hoger dan het aangegeven
aantal mogen worden ge-
stapeld vanwege de aard
van de transportverpakking
of vanwege de aard van de
items zelf.
EN ISO 15223-
1, 5.2.8
ISO 7000, 2606
Niet gebruiken
als de verpak-
king bescha-
digd is
Geeft een medisch hulp-
middel aan dat niet mag
worden gebruikt als de
verpakking beschadigd of
geopend is en dat de ge-
bruiker de gebruiksaanwij-
zing moet raadplegen voor
aanvullende informatie.
Symbool Norm-referen-
tie en sym-
bool-nummer
Titel van sym-
bool Beschrijving van symbool
IEC 60601-1,
Tabel D.1, 8
IEC 60417,
5021
Equipotentiale
aarding
Identificeert de aansluitin-
gen die, indien ze op elkaar
worden aangesloten, de
verschillende onderdelen
van apparatuur of een
systeem naar dezelfde
potentiaal brengen, niet
noodzakelijkerwijs de
aardpotentiaal, bijvoorbeeld
voor lokale vereffening.
AEEA-Richtlijn
2002/96/EC
2012/19/EC
EN 60417,
6414
Richtlijn van de
Europese Unie
inzake Afval
van elektrische
en elektroni-
sche appa-
ratuur (AEEA)
2002/96/EG
Geeft aan dat afgedankte
elektrische en elektroni-
sche apparatuur (AEEA)
afzonderlijk moet worden
ingezameld.
ISO 7010
ISO 3864-2,
M002
Volg de ge-
bruik-saanwij-
zing
Geeft aan dat de gebruiks-
aanwijzing/het instruc-
tieboekje moet worden
gelezen.
IEC 60417,
5114 Bediening met
voetpedaal
Identificeert de
voetschakelaar of de
aansluiting voor een
voetschakelaar.
EN ISO 15223-
1, 5.3.1
ISO 7000, 0621
ISO 780
Breekbaar
Geeft een medisch appa-
raat aan dat kan breken of
beschadigd kan raken als
het niet zorgvuldig wordt
gehanteerd.
IEC 60143-1,
5016 Zekering Identificeert zekeringsdoz-
en of de locatie ervan.
HP N/A Hoge druk Geeft hoge druk aan.
EN ISO 15223-
1, 5.3.8
ISO 7000, 2620
Vochtig-
heids-grens
Geeft de graad van lucht-
vochtigheid aan waaraan
het apparaat veilig kan
worden blootgesteld.
EN ISO 15223-
1, 5.3.2
ISO 7000, 0624
ISO 780
Beschermen
tegen warmte
Geeft een medisch appa-
raat aan dat moet worden
beschermd tegen warmt-
ebronnen.
EN ISO 15223-
1, 5.3.4
ISO 7000, 0626
ISO 780
Droog bewaren Geeft een medisch hulp-
middel aan dat tegen vocht
moet worden beschermd.

28
NEDERLANDS
Symbool Norm-referen-
tie en sym-
bool-nummer
Titel van sym-
bool Beschrijving van symbool
EN ISO 15223-
1, 5.1.1
ISO 7000, 3082
Fabrikant Geeft de fabrikant van het
medische hulpmiddel aan.
ISO/DIS 15223-
1, 5.7.7 Medisch ap-
paraat Geeft aan dat het item een
medisch apparaat is
N/A Geen olie Geeft aan dat er geen olie
aanwezig is.
EN ISO 15223-
1, 5.2.7
ISO 7000, 2609 Non-sterile
Geeft een medisch appa-
raat aan dat geen sterilisa-
tieproces
heeft ondergaan.
LATEX EN ISO 15223-
1, Bijlage B
Niet vervaar-
digd met latex
van natuurlijk
rubber
Geeft aan dat er geen
droog natuurlijk rubber of
latex van natuurlijk rubber
aanwezig is.
ISO 7000, 2794 Verpakking-
seenheid Geeft het aantal items in
een verpakking aan.
FDA 21 CFR
801
Uitsluitend
voorgeschreven
gebruik
Let op: Krachtens federale
wetgeving mag dit hulp-
middel uitsluitend door of
op voorschrift van een arts
worden aangeschaft.
IEC 60417,
5140
Niet-ionise-
rende elektro-
magnet-ische
straling
Geeft algemeen verhoog-
de, mogelijk schadelijke,
niveaus
van niet-ioniserende
straling aan of geeft ap-
paratuur of systemen aan,
bijvoorbeeld op het gebied
van medische elektronica,
die RF-zenders bevatten of
met opzet elektromagneti-
sche RF-straling toepassen
voor diagnosticering of
behandelingen.
EN ISO 15223-
1, 5.1.7
ISO 7000, 2498
Serienummer
Geeft het serienummer
van de fabrikant aan zodat
een specifiek medisch
hulpmiddel kan worden
geïdentificeerd.
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 3707
Enkele steriele
barrière Geeft een enkele steriele
barrière aan. AW-22724-1501 Rev. 001
04/2022
Symbool Norm-referen-
tie en sym-
bool-nummer
Titel van sym-
bool Beschrijving van symbool
EN ISO 15223-
1, 5.2.3
ISO 7000, 2501
Gesteriliseerd
met ethy-
leenoxide
Geeft een medisch
hulpmiddel dat met ethy-
leenoxide gesteriliseerd is.
EN ISO 15223-
1, 5.3.7
ISO 7000, 0632
Temperatuur-li-
miet
Hiermee wordt de tempe-
ratuurlimiet aangegeven
waaraan het apparaat
veilig kan worden bloot-
gesteld.
ISO 7000, 0623
ISO 780, 0623
IATA 2004
Deze kant
boven
Geeft de juiste rechtop-
staande positie van de
transportverpakking aan.
UDI
ISO/DIS 15223-
1, 5.7.10 Unieke appa-
raatidentificatie
Geeft apparaatidentificaties
en productidentificaties
van het medische apparaat
aan.
EN ISO 15223-
1, 5.1.4
ISO 7000, 2607
Vervaldatum
Geeft de datum aan
waarna het hulpmiddel
niet meer mag worden
gebruikt.
Hologic, NovaSure en de bijbehorende logo's zijn handelsmerken en/of
gedeponeerde handelsmerken van Hologic, Inc. en/of dochterbedrijven
van deze onderneming in de Verenigde Staten en/of andere landen.
Het NovaSure endometriumablatiesysteem met impedantieregeling
wordt vervaardigd en gedistribueerd door Hologic, Inc.
© 2014-2022 Hologic, Inc.

1
FRANÇAIS
NovaSure®
Mode d’emploi et manuel de l’opérateur
du contrôleur
Tableau des matières
Liste de contrôle du médecin ..........................1
Description du système ...............................1
Groupe cible de patients ..............................3
Avantages cliniques prévus pour les patients .............3
Utilisateur prévu ....................................3
Indications .........................................3
Contre-indications ................................... 3
Avertissements .....................................4
Précautions d’emploi. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Données cliniques NovaSure sur 3ans ..................6
Événements indésirables ............................. 6
Complications possibles après l’intervention ..............6
Autres événements indésirables .......................7
Étude clinique .....................................7
Sélection des patientes ..............................9
Conseils aux patientes .............................10
Préparation des patientes avant le traitement ............ 10
Mode d’emploi du système d’ablation de l’endomètre
contrôlée par impédance NovaSure ....................10
Fonctionnement du contrôleur RF Modèle 10 ............16
Maintenance périodique et entretien ...................17
Icônes de l’écran du contrôleur RF NovaSure Modèle 10 ......18
Résolution des alarmes les plus courantes ..............18
Résolution des autres problèmes ......................20
Spécifications techniques ............................ 21
Dispositif jetable NovaSure ..........................21
Contrôleur RF NovaSure ............................21
Conditions environnementales ........................ 22
Performances importantes Caractéristiques ..............22
Directives de sécurité électromagnétique ...............22
Nettoyage et désinfection ...........................24
Liste des pièces ..................................25
Élimination ........................................ 25
Garantie ..........................................25
Assistance technique et informations pour le
renvoi du produit ...................................25
Glossaire de symboles ..............................26
MISE EN GARDE: LA LOI FÉDÉRALE (DES ÉTATS-UNIS)
LIMITE LA VENTE DE CE DISPOSITIF PAR UN MÉDECIN
FORMÉ À SON UTILISATION OU SUR ORDONNANCE.
Lire toutes les instructions, toutes les mises en garde et tous les
avertissements avant utilisation. Le non-respect des instructions
ou des avertissements et des précautions d’emploi pourrait blesser
gravement la patiente.
Remarque: le manuel qui accompagne le dispositif jetable peut
contenir une révision plus récente des instructions du système
NovaSure que celle du manuel fourni avec le contrôleur.
Le dispositif jetable NovaSure ne doit pas être utilisé avec d’autres
contrôleurs et/ou générateurs RF. Le contrôleur RF NovaSure ne doit
pas non plus être employé avec d’autres dispositifs jetables.
Le dispositif jetable NovaSure ne contient pas de latex.
Liste de contrôle du médecin
Le médecin doit:
• avoir une expérience suffisante en matière d’interventions dans la
cavité utérine, comme la pose d’un dispositif intra-utérin (DIU) ou la
dilatation et le curetage, avoir suivi une formation adéquate, posséder
les connaissances nécessaires et s’être familiarisé à l’utilisation du
système NovaSure;
• assimiler les instructions du mode d’emploi et suivre une formation
NovaSure ou être formé par un médecin qualifié;
• connaître la séquence appropriée des actions détaillée dans le mode
d’emploi ainsi que dans les sections sur la résolution des problèmes
de ce manuel afin d’interrompre le traitement, d’y mettre fin et/ou
de le poursuivre au cas où le système détecterait une perte de CO2
pendant l’évaluation de l’intégrité de la cavité utérine, qui signale la
possibilité d’une perforation de l’utérus.
Le personnel d’assistance doit être familiarisé avec ces instructions et
les autres documents de formation avant d’utiliser le système NovaSure.
Description du système
Le système d’ablation de l’endomètre contrôlée par impédance
NovaSure est composé du dispositif jetable NovaSure muni de son
cordon de branchement, du contrôleur RF NovaSure (contrôleur), de la
cartouche de CO2 NovaSure, d’un déshydratant, d’une pédale et d’un
cordon d’alimentation, qui sont conçus pour être utilisés ensemble en
tant que système.

2
FRANÇAIS
Dispositif jetable NovaSure avec cordon de branchement,
y compris un déshydratant pour tubulure d’aspiration
Description du dispositif jetable NovaSure
Le dispositif jetable NovaSure comporte une rangée d’électrodes
bipolaires adaptables, à usage unique, montées sur un cadre extensible,
capable de créer une lésion confluente sur la totalité de la surface
intérieure de la cavité utérine. Il s’insère dans la cavité utérine au
travers du col de l’utérus, et la gaine se rétracte pour laisser la rangée
d’électrodes bipolaires se déployer et prendre la forme de la cavité
utérine.
La rangée d’électrodes bipolaires est en tissu poreux métallisé qui aspire
continuellement la vapeur et l’humidité du tissu desséché. Le dispositif
jetable fonctionne en association avec un contrôleur RF NovaSure dédié
pour procéder à l’ablation globale et personnalisée de l’endomètre
en un temps moyen approximatif de 90secondes sans requérir de
visualisation hystéroscopique concomitante ou de traitement préalable
de l’endomètre. La configuration spécifique de la rangée d’électrodes
bipolaires et la puissance prédéterminée du contrôleur créent une
profondeur d’ablation contrôlée dans l’utérus inférieure ou égale à 10cm
et dont la distance minimale entre les cornes est de 2,5cm.
Pendant la procédure d’ablation, le flux de l’énergie de radiofréquence
(RF) vaporise et/ou coagule l’endomètre, quelle que soit son épaisseur, et
dessèche et coagule le myomètre superficiel sous-jacent.
Le contrôleur calcule automatiquement le niveau de puissance optimal
(W) nécessaire au traitement de la cavité utérine en fonction de la taille
de l’utérus. Tandis que la destruction des tissus atteint une profondeur
optimale, l’augmentation de l’impédance tissulaire provoque l’arrêt
automatique de l’administration de puissance par le contrôleur, ce qui
assure une fonction d’autorégulation. Le sang, le sérum physiologique
et tout autre liquide présent dans la cavité utérine au moment de
l’intervention, ainsi que la vapeur produite par les tissus desséchés, sont
évacués par une aspiration automatique continue.
Le dispositif jetable est relié au contrôleur par un cordon qui contient le
câble RF et la tubulure d’aspiration utilisée pour contrôler la pression
pendant le cycle d’évaluation de l’intégrité de la cavité utérine et pour
aspirer pendant le cycle d’ablation. Ce cordon contient aussi la tubulure de
retour de vide utilisée pour administrer le dioxyde de carbone pendant le
cycle d’évaluation de l’intégrité de la cavité utérine et le contrôle du vide
pendant le cycle d’ablation. Le dispositif jetable a été stérilisé à l’oxyde
d’éthylène (OE).
Description du contrôleur RF NovaSure
Le contrôleur RF NovaSure est un générateur de puissance de sortie
constante, doté d’une capacité d’administration de puissance nominale
maximale de 180watts. Le contrôleur calcule automatiquement la
puissance de sortie en fonction des mesures de longueur (mesure de
la profondeur par sondage moins la longueur du canal endocervical)
et de largeur de la cavité utérine que l’utilisateur lui indique au
moyen des touches. Le contrôle de l’impédance tissulaire pendant la
procédure d’ablation permet de réguler automatiquement la profondeur
de l’ablation endo-myométriale. La procédure NovaSure se termine
automatiquement une fois que la vaporisation de l’endomètre et la
dessiccation du myomètre superficielle ont atteint environ 50ohms
d’impédance à l’interface tissu-électrode, ou lorsque la minuterie de
traitement atteint deux minutes. Le système d’évaluation de l’intégrité
de la cavité utérine, conçu pour déceler la présence d’un défaut ou
d’une perforation de la paroi utérine, est intégré au contrôleur. Une fois
le dispositif jetable placé dans la cavité utérine, le CO2 est administré par
la lumière centrale du dispositif jetable dans la cavité par le biais de la
tubulure de retour de vide, à un débit et une pression sûrs. Si la pression
de CO2 dans la cavité se maintient pendant une courte durée, indiquant
que la cavité utérine est intacte, le système d’évaluation de l’intégrité de
la cavité utérine permet alors l’activation du contrôleur RF NovaSure afin
de procéder au traitement. Une pompe à vide placée dans le contrôleur
RF NovaSure crée et maintient le vide dans la cavité utérine pendant
toute l’intervention d’ablation de l’endomètre. Une fois le vide stabilisé,
le niveau de vide est surveillé pendant tout le reste de laprocédure
d’ablation.
Contrôleur RF NovaSure
Modèle 10

3
FRANÇAIS
Description du déshydratant pour
tubulure d’aspiration NovaSure
Le déshydratant pour tubulure
d’aspiration NovaSure est un composant
non stérile à usage unique qui se fixe
dans le prolongement de la tubulure
d’aspiration avant de relier le dispositif
jetable au contrôleur RF NovaSure.
Le déshydratant absorbe l’humidité
retirée de la cavité utérine par le biais
de la tubulure d’aspiration pendant la
procédure d’ablation.
Description de la pédale NovaSure
La pédale NovaSure est un commutateur
pneumatique relié au panneau avant
du contrôleur RF NovaSure. Elle permet
d’activer le contrôleur RF NovaSure et
ne contient aucun composant électrique.
Description de la cartouche de
CO2 NovaSure
La cartouche de CO2 NovaSure contient
16grammes de CO2 (Pharmacopée
américaine ou USP). Elle est reliée au
détendeur situé sur le panneau arrière
du contrôleur RF NovaSure avant de
mettre ce dernier sous tension. Le CO2
est utilisé par le système d’évaluation
de l’intégrité de la cavité utérine afin
demettre celle-ci sous pression.
La cartouche de CO2 réf: 815012 est
99% de CO2
Description du cordon
d’alimentation secteur NovaSure
Le cordon d’alimentation secteur
NovaSure est un cordon de qualité
médicale qui relie le contrôleur
RF NovaSure à la tension secteur
appropriée. La prise pour le cordon
d’alimentation, le module d’arrivée
dusecteur, se trouve sur le panneau
arrière du contrôleur RF NovaSure.
Indications
Le système NovaSure est conçu pour l’ablation de l’endomètre qui
recouvre l’intérieur de l’utérus chez les femmes en préménopause
souffrant de ménorragie (saignements excessifs) due à des causes
bénignes et ne devant plus avoir d’enfant.
Groupe cible de patients
Le système NovaSure est destiné à être utilisé sur les femmes pré-
ménopausées avec ménorragie (saignement excessif) due à des causes
bénignes pour lesquelles la procréation est terminée.
Avantages cliniques prévus pour les patients
Réduire ou éliminer les saignements chez les femmes pré-ménopausées
avec des saignements menstruels importants dus à des causes bénignes
pour lesquelles la procréation est terminée.
Utilisateur prévu
Le système NovaSure sera utilisé sous le contrôle et les consignes
d’un médecin OB/GYN ou d’un médecin ou chirurgien GYN. Le médecin
sera l’utilisateur principal du dispositif NovaSure et peut fournir des
instructions à l’assistant sur le fonctionnement du contrôleur RF et
activer le contrôleur à l’aide de l’interrupteur au pied. Le contrôleur RF
sera actionné par un assistant non stérile.
Le médecin doit:
• Avoir une expérience suffisante dans l’exécution de procédures
dans la cavité utérine, telle que l’insertion IUD ou la dilatation et le
curetage (D&C) et avec une formation, des connaissances et une
familiarité adéquates à l’utilisation du système NovaSure.
• Passer en revue et connaître les instructions et effectuer soit la
formation NovaSure ou être formé par un médecin qualifié.
Le personnel auxiliaire doit connaître le mode d’emploi et
les autres supports de formation avant d’utiliser le système NovaSure.
Contre-indications
Le système d’ablation de l’endomètre contrôlée par impédance
NovaSure est contre-indiqué dans les cas suivants:
• patiente enceinte ou souhaitant l’être. Les grossesses suivant
l’ablation peuvent s’avérer dangereuses pour la mère et le fœtus.
• patiente présentant un carcinome de l’endomètre avéré ou suspecté
(cancer de l’utérus) ou présentant des conditions précancéreuses de
l’endomètre (par exemple, hyperplasie adénomateuse non résolue).
• patiente ayant un problème anatomique (par exemple, des antécédents
de césarienne classique ou de myomectomie transmurale) ou
pathologique (par exemple, un traitement médical à long terme) qui
risquerait d’affaiblir le myomètre.
• patiente présentant une infection active des voies génitales ou
urinaires au moment de l’intervention (par exemple, cervicite, vaginite,
endométrite, salpingite ou cystite).
• patiente porteuse d’un dispositif intra-utérin (DIU). La présence d’un
DIU dans la cavité utérine peut interférer avec la procédure NovaSure.
• patiente dont la cavité utérine mesure moins de 4cm de long. La
longueur minimale de la rangée d’électrodes est de 4cm. Le traitement
d’une cavité utérine d’une longueur inférieure à 4 cm provoquerait des
brûlures au niveau du canal endocervical.
• patiente dont la cavité utérine mesure moins de 2,5cm de large, telle
que déterminée par le cadran WIDTH (LARGEUR) du dispositif jetable,
suite à son déploiement.
• patiente souffrant d’une inflammation pelvienne active.

4
FRANÇAIS
• Un risque peut exister pour la santé lorsque la procédure NovaSure est
effectuée en présence d’un micro-implant métallique thermoconducteur
et électroconducteur mal positionné (par exemple, perforant la trompe
de Fallope ou le myomètre). Si cela se produit, la chaleur peut être
détournée de la zone de traitement visée vers d’autres tissus et/
ou organes en contact avec l’objet conducteur, ce qui peut suffire
à provoquer des brûlures localisées. Par conséquent, il convient
de vérifier le positionnement du micro-implant métallique avant
d’effectuer la procédure NovaSure.
Aspects techniques
• Ne pas utiliser le dispositif jetable stérile à usage unique si son
emballage est endommagé ou si sa stérilité a pu être compromise.
• Le dispositif jetable est exclusivement à usage unique. Ne pas le
réutiliser ou le restériliser. Les risques liés à une réutilisation du
dispositif jetable incluent notamment ce qui suit :
• procédure inefficace ;
• infection (majeure) ;
• choc électrique ;
• transmission d’une maladie contagieuse ;
• lacération du col de l’utérus ;
• perforation de l’utérus.
• Si une procédure hystéroscopique est effectuée avec une solution
hypotonique juste avant le traitement NovaSure, la cavité utérine doit
alors être rincée avec du sérum physiologique avant de procéder
au traitement avec le système NovaSure. La présence de liquide
hypotonique peut réduire l’efficacité du système NovaSure.
• Le branchement du dispositif jetable sur le contrôleur lance
l’administration de CO2 afin de purger tout l’air du dispositif jetable et
de la tubulure. Cette opération de purge prend environ 10secondes et
doit s’effectuer lorsque le dispositif jetable se trouve à l’extérieur
de la patiente pour éliminer tout risque d’aéroembolisme ou
d’embolie gazeuse. Un message de purge du dispositif s’affiche sur le
modèle 10RFC et une tonalité pulsée audible retentit tout au long de la
procédure de purge. Lorsque le bip sonore s’arrête et que la DEL s’éteint
ou le message à l’écran disparaît, le dispositif jetable peut être inséré en
toute sécurité.
• Pour les patientes portant un stimulateur cardiaque ou d’autres implants
actifs, il existe un risque d’interférences avec le fonctionnement du
stimulateur pouvant endommager ce dernier. Consulter le fabricant du
stimulateur pour plus de détails en cas d’utilisation prévue du système
NovaSure sur des patientes portant un stimulateur cardiaque.
• Prendre les précautions appropriées pour s’assurer que la patiente
n’entre pas en contact avec les parties métalliques qui sont reliées
àla terre ou qui ont une capacité appréciable par rapport à la terre.
• Danger: risque d’explosion. Ne pas utiliser en présence d’un
mélange anesthésique inflammable. Ne pas utiliser en présence de
gaz ou de liquides inflammables.
• Une défaillance du contrôleur RF NovaSure pourrait provoquer une
augmentation involontaire de la puissance de sortie.
Avertissements
Le non-respect des instructions ou des avertissements et des
mises en garde pourrait blesser gravement lapatiente.
Le dispositif jetable NovaSure doit être uniquement utilisé en
association avec le contrôleur RF NovaSure.
La procédure NovaSure est conçue pour être effectuée une
seule fois pendant une consultation opératoire unique. Des
brûlures à l’intestin peuvent se produire lorsque plusieurs
cycles de traitement NovaSure sont effectués lors d’une même
consultation opératoire.
Perforation de l’utérus
• Veiller à ne pas perforer la paroi utérine lors de la mesure par
sondage, de la dilatation ou de l’insertion du dispositif jetable.
• Si le dispositif jetable est difficile à insérer dans le canal cervical,
utiliser son jugement clinique pour déterminer si une dilatation plus
poussée est nécessaire.
• Le système NovaSure effectue une évaluation de l’intégrité de la cavité
utérine et émet une alarme sonore d’alerte de perforation possible
avant le traitement (étape 2.36). (Bien que conçu pour détecter une
perforation de la paroi utérine, il s’agit seulement d’un indicateur
qui pourrait ne pas déceler toutes les perforations dans toutes
les circonstances possibles. Toujours faire appel à son jugement
clinique.)
• En cas de suspicion d’une perforation de l’utérus, l’intervention
doit être immédiatement interrompue.
• Si l’évaluation de l’intégrité de la cavité utérine échoue après des
tentatives raisonnables d’exécution des procédures de résolution
des problèmes (étape 2.36), interrompre l’intervention.
• Chez les patientes dont l’intervention a été interrompue en raison
d’une suspicion de perforation de la paroi utérine, une investigation de
la perforation doit être envisagée avant la sortie de l’hôpital.
Généralités
• L’ablation de l’endomètre au moyen du système NovaSure ne
constitue pas une procédure de stérilisation. Il convient donc
d’indiquer à la patiente les méthodes de contraception appropriées.
• L’ablation de l’endomètre n’élimine pas les risques d’hyperplasie ou
d’adénocarcinome de l’endomètre, et peut empêcher le médecin de
détecter ou de diagnostiquer une telle pathologie.
• L’ablation de l’endomètre est uniquement indiquée chez les femmes
qui ne souhaitent pas avoir d’enfants, car elle réduit significativement
les possibilités de grossesse. Une grossesse suivant l’ablation peut
s’avérer dangereuse pour la mère et le fœtus.
• Les patientes qui subissent une procédure d’ablation de l’endomètre
après une ligature des trompes risquent davantage de développer un
syndrome de stérilisation tubaire post-ablation qui pourrait nécessiter
une hystérectomie. Ceci peut se produire jusqu’à 10ans après
l’intervention.

5
FRANÇAIS
Précautions D’Emploi
• Il a été signalé dans des publications scientifiques que les patientes
ayant une antéversion, une rétroflexion ou un déplacement latéral
sévères de l’utérus risquent davantage de subir une perforation de la
paroi utérine pendant une manipulation intra-utérine.
• Un faux passage peut se produire pendant toute intervention
impliquant la manipulation d’instruments dans l’utérus, surtout dans
les cas d’antéversion, de rétroflexion ou de déplacement latéral
sévères de l’utérus. Procéder avec précaution pour s’assurer que le
dispositif est correctement positionné dans la cavité utérine.
• Le système NovaSure se compose des éléments suivants:
- dispositif jetable NovaSure à usage unique avec cordon de
branchement;
- contrôleur RF NovaSure ;
- cartouche de CO2 NovaSure;
- déshydratant NovaSure;
- pédale NovaSure;
- cordon d’alimentation.
Pour garantir un fonctionnement correct, ne jamais utiliser d’autres
composants avec le système NovaSure. Examiner régulièrement les
éléments afin de déceler toute détérioration éventuelleet ne pas les
utiliser en cas de détérioration apparente. L’utilisation de câbles ou
d’accessoires autres que ceux indiqués dans ces instructions pourrait
provoquer une augmentation des émissions ou une réduction de
l’immunité du contrôleur RF.
• Le contrôleur RF doit être installé et mis en service conformément aux
conseils fournis dans ces instructions pour garantir sa compatibilité
électromagnétique. Consulter les tableaux d’émissions électromagnétiques
et d’immunité électromagnétique à la section Caractéristiques techniques.
• Le contrôleur RF ne doit pas être utilisé à proximité d’un autre appareil
ou posé dessus. S’il doit être utilisé à proximité d’un autre appareil
ou posé dessus, le fonctionnement normal du contrôleur RF doit être
vérifié dans la configuration dans laquelle il doit être utilisé.
• Des équipements de communication RF mobiles et portables peuvent
affecter le contrôleur RF. Consulter les distances de séparation
recommandées dans les tableaux d’immunité électromagnétique à la
section Caractéristiques techniques.
• Pour les patientes ayant subi une ablation de l’endomètre et qui sont
ultérieurement placées sous hormonothérapie substitutive, il convient
de prescrire également un progestatif afin d’éviter les risques accrus
d’adénocarcinome de l’endomètre associés à une œstrogénothérapie
substitutive non compensée.
• L’innocuité et l’efficacité du système NovaSure n’ont pas été
entièrement évaluées chez les patientes:
- avec une mesure de sondage de l’utérus supérieure à 10cm ;
- avec des fibromes sous-muqueux déformant la cavité utérine ;
- avec un utérus bicorne, cloisonné ou sous-bifide ;
- sous prétraitement médical (par exemple, antagoniste de la GnRH)
ou chirurgical;
- qui ont subi une ablation préalable de l’endomètre, y compris au
moyen de la procédure d’ablation NovaSure; ou
- qui sont ménopausées.
• Ne pas essayer de réparer le contrôleur en cas de suspicion
de problèmes. Appeler l’assistance technique d’Hologic ou un
représentant commercial d’Hologic pour obtenir des instructions.
• Les câbles du dispositif jetable doivent être placés de manière à éviter
tout contact avec la patiente ou toute autre dérivation.
• L’utilisateur doit examiner le dispositif jetable afin de déceler toute
détérioration éventuelle avant utilisation.
• Le déshydratant pour tubulure d’aspiration est non stérile et son
emballage ne doit pas être placé dans le champ stérile.
• Si un message de position ARRAY s’affiche sur l’écran du modèle10,
voir la section Dépannage sous «ALARME DE POSITION ARRAY».
• Ne pas utiliser le déshydratant pour tubulure d’aspiration NovaSure si
le produit est de couleur rose.
• Le dispositif jetable doit se trouver en dehors de la patiente lors du
branchement du cordon sur la prise correspondante du panneau avant
du contrôleur (étape 2.15).
• La cartouche de dioxyde de carbone contient du gaz sous haute
pression. Si une cartouche de CO2 ou sa tubulure est percée, laisser
la cartouche se vider complètement et laisser la cartouche et/ou la
tubulure s’équilibrer à température ambiante avant de les manipuler.
• Le CO2 s’écoule continuellement à partir du moment où le dispositif
jetable est branché sur le contrôleur jusqu’à ce que le test d’évaluation
de l’intégrité de la cavité utérine de la procédure soit terminé. Pour
réduire la durée d’administration du CO2 et les risques d’embolie,
effectuer la procédure de positionnement immédiatement après avoir
inséré le dispositif jetable et passer directement de la procédure de
positionnement à l’évaluation de l’intégrité de la cavité utérine.
• Les objets électroconducteurs (par exemple, électrodes de monitorage
d’autres appareils) qui sont en contact direct avec la rangée d’électrodes
du dispositif jetable, ou se trouvant très près, risquent de détourner
du courant de la rangée d’électrodes. Ceci risque de produire des
brûlures localisées sur la patiente ou le médecin, ou de déformer
le champ électrique de la rangée d’électrodes, et de modifier ainsi
l’effet thérapeutique (traitement trop faible ou trop fort). Cela pourrait
également déformer le courant au niveau de l’objet conducteur, les
moniteurs risquant par exemple d’afficher des mesures erronées.
• La mise à la terre est fiable uniquement lorsque l’appareil est branché
sur une prise portant la mention «de qualité hospitalière».
• Pour éviter tout risque pour la patiente et les opérateurs, ne pas utiliser
cet équipement en présence de sources magnétiques, de source
d’ultrasons ou de sources de chaleur intentionnelles.
• Le collier cervical doit être complètement rétracté jusqu’à sa position
proximale de manière à réduire au maximum le risque de détérioration
de la gaine lors de la fermeture de la rangée d’électrodes.
• L’utilisation du dispositif NovaSure est contre-indiquée chez les
femmes enceintes ou chez les femmes qui aimeraient le devenir. Une
grossesse faisant suite à une ablation peut être dangereuse pour la
maman et le foetus. Faire preuve d’un bon jugement médical.

6
FRANÇAIS
Données cliniques NovaSure sur 3ans
Événements indésirables
Le système NovaSure a été évalué lors d’une étude clinique
multicentrique prospective randomisée incluant 265patientes souffrant
de saignements utérins anormaux et comparant le système NovaSure
à un bras témoin avec résection de l’endomètre à l’anse suivie d’une
ablation par Rollerball.
Tableau 1A. Événements indésirables peropératoires
Événement indésirable
NovaSure
n=175 (%)
Résection à l’anse
plus Rollerball
n=90 (%)
Bradycardie 1 (0,6 %) 0 (0,0 %)
Perforation de l’utérus 0 (0,0 %) 3 (3,3 %)
Déchirure cervicale 0 (0,0 %) 2 (2,2 %)
Sténose cervicale 0 (0,0 %) 1 (1,1 %)
TOTAL 1 (0,6 %) 6 (6,7 %)
Tableau 1B. Événements indésirables post-opératoires <24 heures
Événement indésirable
NovaSure
n=175 (%)
Résection à l’anse
plus Rollerball
n=90 (%)
Douleurs/Crampes pelviennes 6 (3,4 %) 4 (4,4 %)
Nausées et/ou vomissements 3 (1,7 %) 1 (1,1 %)
TOTAL 9 (5,1 %)* 5 (5,6 %)**
* Neuf événements signalés chez 6 (3,4%) patientes
** Cinq événements signalés chez 4 (4,4%) patientes
Tableau1C. Événements indésirables post-opératoires
>24 heures – 2 semaines
Événement indésirable
NovaSure
n=175 (%)
Résection à l’anse
plus Rollerball
n=90 (%)
Hématométrie 1 (0,6 %) 0 (0,0 %)
Infection des voies urinaires 1 (0,6 %) 1 (1,1 %)
Infection vaginale 1 (0,6 %) 0 (0,0 %)
Endométrite 0 (0,0 %) 2 (2,2 %)
Inflammation pelvienne 0 (0,0 %) 1 (1,1 %)
Hémorragie 0 (0,0 %) 1 (1,1 %)
Douleurs/Crampes pelviennes 1 (0,6 %) 1 (1,1 %)
Nausées et/ou vomissements 1 (0,6 %) 1 (1,1 %)
TOTAL 5 (2,9 %)* 7 (7,8 %)**
* Cinq événements signalés chez 4 (2,3%) patientes
** Sept événements signalés chez 6 (6,7%) patientes
Tableau 1D. Événements indésirables post-opératoires
>2 semaines – 1 an
Événement indésirable
NovaSure
n=175 (%)
Résection à l’anse
plus Rollerball
n=90 (%)
Hystérectomie 3 (1,7 %) 2 (2,2 %)
Hématométrie 1 (0,6 %) 2 (2,2 %)
Infection des voies urinaires 2 (1,1 %) 2 (2,2 %)
Infection vaginale 5 (2,9 %) 2 (2,2 %)
Endométrite 2 (1,1 %) 1 (1,1 %)
Inflammation pelvienne 2 (1,1 %) 0 (0,0 %)
Hémorragie 1 (0,6 %) 0 (0,0 %)
Douleurs/Crampes pelviennes 5 (2,9 %) 6 (6,7 %)
TOTAL 21 (12,0 %)* 15 (16,17 %)**
* 21 événements chez 19 (10,9%) patientes
** 15 événements chez 15 (16,7%) patientes
Complications possibles après l’intervention
Pour toute procédure d’ablation de l’endomètre, les événements post-
opératoires communément signalés sont les suivants:
• crampes/douleurs pelviennes signalées chez 3,4% des patientes
NovaSure et 4,4% des patientes traitées par résection à l’anse plus
Rollerball dans les 24 heures suivant l’intervention. Les crampes
post-opératoires vont de légères à sévères. Ces crampes durent
normalement quelques heures et persistent rarement après le premier
jour suivant l’intervention.
• nausées et vomissements signalés chez 1,7% des patientes NovaSure
et 1,1% des patientes traitées par résection à l’anse plus Rollerball
dans les 24heures suivant l’intervention. Lorsqu’ils se produisent, les
nausées et les vomissements surviennent généralement juste après
l’intervention, sont associés à l’anesthésie et peuvent être traités par
des médicaments.
• pertes vaginales.
• saignements vaginaux/pertes vaginales légères.
Autres événements indésirables
Comme dans toutes les procédures d’ablation de l’endomètre, des
blessures graves, voire mortelles, peuvent se produire.
Les événements indésirables suivants peuvent se produire, ou ont été
signalés, en association avec l’utilisation du système NovaSure:
• syndrome de stérilisation tubaire post-ablation;
• complications liées à une grossesse (remarque: toute grossesse
suivant une ablation de l’endomètre est trèsdangereuse pour
la mère comme pour le fœtus);
• brûlures des tissus adjacents;
• perforation de la paroi utérine;
• difficultés de selle ou de miction;
• nécrose utérine;
• aéroembolisme ou embolie gazeuse;
• infection ou septicémie;
• complications entraînant des blessures graves ou le décès.

7
FRANÇAIS
Étude clinique
Objectif: l’innocuité et l’efficacité de l’utilisation du système NovaSure
ont été comparées à celles de la résection de l’endomètre à l’anse suivie
de l’ablation par Rollerball chez des femmes en préménopause souffrant
de ménorragie suite à des causes bénignes.
Traitement préalable: les patientes randomisées dans le bras NovaSure
n’ont reçu aucun traitement endométrial préalable (par exemple, hormone,
dilatation-curetage ou synchronisation de la patiente). Les patientes
randomisées dans le bras témoin ont subi une résection à l’anse comme
traitement endométrial préalable.
Critères d’évaluation de l’étude: la mesure d’efficacité principale
consistait en un système de score menstruel validé sur journal mis au point
par Higham (Higham JM, O’Brien PMS, Shaw RW Br J Obstet Gynaecol
1990; 97:734-9). L’évaluation des pertes de sang menstruel a été effectuée
à l’aide d’un graphique figuratif d’évaluation des pertes sanguines (PBLAC).
La réussite au niveau des patientes a été définie comme une réduction
des écoulements menstruels à 1an après l’intervention, atteignant un
score sur journal <75. La réussite au niveau de l’étude a été définie
comme étant une différence statistique inférieure à 20% dans les taux
de réussite des patientes entre le système d’ablation de l’endomètre
contrôlée par impédance NovaSure et la résection à l’anse suivie d’une
ablation par Rollerball. Les patientes ont été contactées à deux et trois ans
et interrogées sur leurs saignements au cours des 12mois précédents.
Lessaignements menstruels de chaque patiente ont été déterminés à deux
et trois ans en utilisant le score PBLAC et le profil de saignement à un an
comme référence. Il a donc été possible de comparer directement le profil
de saignement ou les saignements menstruels d’une patiente à un an au
profil de saignement à deux et trois ans.
Les critères d’évaluation secondaires comprenaient le mode d’anesthésie,
la durée de l’intervention et les réponses à un questionnaire sur la
qualité de vie. L’évaluation de l’innocuité a été basée sur les événements
indésirables signalés pendant l’étude.
Méthodes: une étude clinique prospective randomisée (2:1) a été
effectuée dans 9sites cliniques et incluait 265patientes avec un diagnostic
de ménorragie. Les scores menstruels sur journal ont été recueillis avant
l’intervention et tous les mois pendant 12mois après l’intervention.
Les patientes ont été traitées à tout moment de leur cycle menstruel.
Aucune patiente n’a reçu de traitement hormonal préalable visant à
réduire l’épaisseur de l’endomètre. Les patientes du bras témoin ont subi
une résection de l’endomètre à l’anse hystéroscopique comme moyen
mécanique de prétraitement de l’endomètre, suivie d’une ablation par
Rollerball. Les sujets de l’étude devaient remplir les principaux critères de
sélection suivants:
Critères d’inclusion
• Ménorragie réfractaire sans cause organique définissable (saignement
utérin dysfonctionnel)
• Âgées de 25 à 50ans
• Mesure par sondage de l’utérus de 6,0 à 10,0cm (de l’orifice externe
au fond interne)
• Score PBLAC minimum >150 pendant 3mois avant l’inclusion à
l’étude; ou score PBLAC >150 pendant un mois pour les femmes avec :
- échec (documenté)du traitement médical au moins pendant les
3mois précédents ;
- contre-indication au traitement médical; ou
- refus du traitement médical.
Critères d’exclusion
• Présence de bactériémie, septicémie ou autre infection systémique active
• Inflammation pelvienne active ou chronique récurrente
• Patiente avec coagulopathies documentées ou sous anticoagulants
• Endométriose symptomatique
• Chirurgie antérieure de l’utérus (sauf césarienne au niveau du
segment inférieur) qui aurait affecté l’intégrité de la paroi utérine,
parexemple, myomectomie transmurale ou césarienne classique
• Ablation antérieure de l’endomètre
• Patiente sous médicaments susceptibles de réduire le muscle du
myomètre, comme l’usage de stéroïdes à long terme
• Patiente souhaitant avoir des enfants ou souhaitant rester fertile
• Patiente sous traitement contraceptif hormonal ou refusant d’utiliser
un contraceptif non hormonal après l’ablation
• Cavité anormale/obstruée confirmée par hystéroscopie,
hystéroéchographie ou hystérosalpingographie. Plusprécisément:
- utérus cloisonné ou bicorne ou autre malformation congénitale de
lacavité utérine;
- léiomyomes sous-muqueux pédiculés ou autres léiomyomes qui
déforment la cavité; polypes (d’une taille supérieure à 2cm) qui
risquent de causer la ménorragie de la patiente;
- présence d’un DIU.
• Malignité utérine suspectée ou confirmée au cours des cinq dernières
années, telle que confirmée par l’histologie
• Hyperplasie endométriale telle que confirmée par l’histologie
• Dysplasie cervicale non traitée
• Taux de FSH élevés concordant avec un problème ovarien >40 UI/ml
• Grossesse
• Maladie sexuellement transmissible active
Population de patientes: au total, 265patientes ont été incluses dans
cette étude. Elles étaient âgées de 25 à 50ans; 46% d’entre elles
avaient moins de 40ans et 54% avaient 40ans ou plus. Il n’existait
aucune différence au niveau des caractéristiques démographiques ou des
antécédents gynécologiques entre les groupes de traitement, les tranches
d’âges ou les neuf sites de l’étude.

8
FRANÇAIS
Tableau 2. Comptabilisation des patientes
Nombre de patientes NovaSure Résection à l’anse
plus Rollerball
Entrées dans l’étude
(population en intention de traiter) 175 90
Procédures interrompues*1-4 -2
Traitées 171 88
Traitement supplémentaire* -4 -2
Hystérectomie*2-3 -2
Perdues de vue* -5 -2
Maladie de Hodgkin* -1 0
Douleurs pelviennes - leuprolide
administré*
-1 0
Données de suivi disponibles à 12mois
157 82
Traitement supplémentaire* -2 -1
Hystérectomie*2-3 -1
Perdues de vue* -2 -5
Visite manquée -1 -1
Refus de participer* -1 0
Grossesse* -1 0
Données de suivi disponibles à 24mois
147 74
Traitement supplémentaire* 0 -4
Hystérectomie*2-5 -1
Perdues de vue* -4 -2
Suivi à 36mois 138 67
Sujet perdu de vue à 24mois, de
retour à 36mois
+1 +1
Données de suivi disponibles à 36mois
139 68
* Patientes sorties de l’étude
1 Quatre patientes NovaSure ne répondaient pas aux critères d’inclusion du protocole; deux patientes
Rollerball ont présenté une perforation de l’utérus
2 Pour l’hystérectomie, voir le tableau7
Résultats
Critère principal d’évaluation de l’efficacité: score des saignements
La réussite pour les patientes à 12mois après l’intervention est définie
comme une réduction du score sur journal de >150 avant l’intervention
à <75 après l’intervention. L’aménorrhée est définie comme étant un
score de 0. La réussite à 24 et 36mois, basée sur les questionnaires
téléphoniques, est définie comme étant l’élimination des saignements
ou une réduction à des écoulements légers ou normaux. Les données
du tableau3 (ci-dessous) représentent les résultats cliniques basés sur
le nombre total des 265patientes randomisées (groupe en intention
de traiter [ITT]) pour l’étude. La pire éventualité a été retenue en
considérant les patientes sorties de l’étude (décrites dans le tableau2
pour la comptabilisation des patientes) comme des «échecs» pour le
calcul des valeurs du tableau.
Tableau3. Efficacité: Taux de réussite – Patientes en intention
detraiter
NovaSure
(n=175)
Résection à l’anse
plus Rollerball
(n=90)
Mois après l’ablation 12* 24** 36** 12* 24** 36**
Nombre de réussites 136 143 134 67 68 63
Taux de réussite
del’étude 77,7 % 81,7 % 76,6 % 74,4 % 75,6 % 70,0 %
Nbre de patientes
avec aménorrhée 63 64 58 29 26 23
Taux d’aménorrhée 36,0 % 36,6 % 33,1 % 32,2 % 28,9 % 25,6 %
* D’après les scores sur journal
** D’après les questionnaires téléphoniques
Critère secondaire d’évaluation de l’efficacité: qualité de vie
La qualité de vie (QdV) des patientes a été évaluée en administrant le
questionnaire de qualité de vie (SF-12) et le questionnaire d’impact
menstruel avant le traitement et à 3, 6, 12, 24 et 36mois après
l’intervention. Le tableau4 présente les réponses des patientes pour les
deux groupes avant l’intervention, le cas échéant, et à 12, 24 et 36après
l’intervention.
Tableau4. Efficacité: qualité de vie (QdV)
NovaSure Résection à l’anse
plus Rollerball
Nombre de patientes ayant répondu au questionnaire sur la qualité de vie#
Avant l’intervention 175 90
12 mois 154 82
24 mois 143 73
36 mois 139 67
Pourcentage de patientes satisfaites ou très satisfaites
12 mois 92,8 % 93,9 %
24 mois 93,9 % 89,1 %
36 mois 96,3 % 89,7 %
Pourcentage de patientes qui recommanderaient probablement ou
certainement cette intervention
12 mois 96,7 % 95,9 %
24 mois 96,6 % 94,5 %
36 mois 97,8 % 92,6 %
Pourcentage de patientes atteintes de dysménorrhée
Avant l’intervention 57,1 % 55,6 %
12 mois 20,8 %& 34,2 %*,&
24 mois 20,3 %* 30,1 %*
36 mois 17,3 %* 28,4 %*
Pourcentage de patientes atteintes du syndrome prémenstruel (SPM)
Avant l’intervention 65,1 % 66,7 %
12 mois 36,4 %* 35,4 %*
24 mois 44,0 %* 46,6 %*
36 mois 34,5 %* 41,2 %*

9
FRANÇAIS
Tableau4. Efficacité: qualité de vie (QdV)
NovaSure Résection à l’anse
plus Rollerball
Pourcentage de patientes signalant avoir parfois, fréquemment ou
toujours des difficultés à effectuer leur travail ou d’autres activités en
raison des règles
Avant l’intervention 66,3 % 65,5 %
12 mois 9,9 %* 8,6 %*
24 mois 14,5 %* 15,0 %*
36 mois 16,3 %* 13,3 %*
Pourcentage de patientes signalant avoir parfois, fréquemment ou
toujours une anxiété en raison des règles
Avant l’intervention 74,7 % 68,9 %
12 mois 23,6 %* 18,5 %*
24 mois 24,2 %* 19,2 %*
36 mois 18,7 %* 19,1 %*
Pourcentage de patientes signalant manquer parfois, fréquemment ou
toujours des activités sociales en raison des règles
Avant l’intervention 63,3 % 62,2 %
12 mois 8,5 %* 8,6 %*
24 mois 9,0 %* 11,1 %*
36 mois 8,1 %* 10,8 %*
# Toutes les patientes n’ont pas rempli le questionnaire
* Différence statistiquement significative par rapport à la réponse avant l’intervention (chicarré; p <0,05)
& Différence statistiquement significative entre les groupes NovaSure et Rollerball (chi carré; p=0,02)
Critère d’évaluation de l’innocuité
Les informations sur les événements indésirables sont décrites dans la
section «Événements indésirables» de ce manuel.
Critère d’évaluation secondaire: durée de l’intervention
La durée de l’intervention, qui constitue un critère d’évaluation
secondaire, a été déterminée pour chaque patiente en enregistrant
l’heure de l’insertion et du retrait du dispositif. La durée moyenne de
l’intervention pour les patientes NovaSure a été significativement plus
courte que pour les patientes du groupe Rollerball, (respectivement
4,2± 3,5 minutes et 24,2 ± 11,4 minutes). La durée moyenne
d’application de l’énergie RF était de 84,0 ± 25,0 secondes pour un
sous-groupe de patientes NovaSure contrôlées (tableau 5).
Tableau5. Durée de l’intervention
Paramètres pris en compte NovaSure
n=175
Résection à l’anse
plus Rollerball
n=90
Nombre de patientes traitées* 171 88
Durée de l’intervention en minutes
(± ET)
(de l’insertion au retrait du dispositif)
4,2 ± 3,5** 24,2 ± 11,4**
Durée de l’intervention en minutes
(± ET)
(durée de l’administration d’énergie)
84,0 ± 25,0 ND#
* Consulter le tableau2 pour connaître la comptabilisation des patientes
** Différence statistiquement significative entre les groupes de traitement (test de Student; p <0,05)
# Non déterminé
Critère d’évaluation secondaire: mode d’anesthésie
L’anesthésie a été laissée à la discrétion de chaque patiente, de chaque
investigateur clinique et de chaque anesthésiste. Parmi les patientes
NovaSure, 27,0% (47/174) ont subi l’intervention sous anesthésie
générale ou épidurale, et 73,0% (127/174) sous anesthésie locale et/ou
sédation par injection IV. Une patiente n’a pas eu de mode d’anesthésie
signalé dans ce groupe. Dans le groupe Rollerball, 82,2% (74/90) des
patientes ont été traitées sous anesthésie générale ou épidurale, et 17,8%
(16/90) sous anesthésie locale et/ou sédation par injection IV (tableau 6).
Tableau6. Mode d’anesthésie
NovaSure
n=175*
Résection à l’anse
plus Rollerball
n=90
Générale ou épidurale 27,0 % 82,2 %
Locale et/ou sédation parinjection IV 73,0 % 17,8 %
* Pour une patiente, aucun mode d’anesthésie n’a été signalé.
Observations cliniques
Hystérectomie
Quinze femmes ont subi une hystérectomie dans les trois ans suivant
la procédure d’ablation. Le tableau7 donne la liste des raisons de
l’hystérectomie.
Tableau7. Hystérectomie
Raison de l’hystérectomie NovaSure
n=175
Résection à l’anse
plus Rollerball
n=90
Adénocarcinome diagnostiqué au
moment de la procédure d’ablation 1 1
Fibromes 2 0
Abcès pelvien 1 1
Endométriose 3 0
Adénomyose 4 0
Hématométrie 0 1
Ménorragie 0 1
TOTAL 11 (6,3 %) 4 (4,4 %)
7 hystérectomies sur des patientes de moins de 40ans (7 NovaSure) et 8 hystérectomies sur des patientes
de plus de 40ans (4 NovaSure et 4 Rollerball).
Sélection des patientes
La ménorragie peut être provoquée par divers problèmes sous-jacents,
notamment, sans toutefois s’y limiter, un cancer de l’endomètre, des
myomes, des polypes, des médicaments et des saignements utérins
dysfonctionnels (saignements anovulatoires). Les patientes doivent
toujours être dépistées et évaluées afin de déterminer la cause de
tout saignement utérin excessif avant d’entreprendre une option
thérapeutique quelconque. Consulter la documentation médicale portant
sur les diverses techniques d’ablation de l’endomètre, les indications, les
contre-indications, les complications et les risques, avant de procéder à
une procédure d’ablation de l’endomètre.

10
FRANÇAIS
Conseils aux patientes
Comme pour toute intervention, le médecin doit discuter des risques,
des avantages et des alternatives avec la patiente, avant de procéder
à l’ablation de l’endomètre. Les patientes doivent comprendre que le
traitement a pour objectif de réduire les saignements à des niveaux
normaux.
Le dispositif jetable est uniquement indiqué chez les femmes qui
ne souhaitent pas avoir d’enfants, car cette intervention réduit
significativement les possibilités de grossesse. Les patientes susceptibles
de tomber enceintes doivent être informées des complications potentielles
en cas de grossesse. Ces conseils doivent comprendre le besoin d’une
contraception après l’intervention, le cas échéant. Cette intervention ne
constitue pas une procédure de stérilisation et toute grossesse ultérieure
pourrait s’avérer dangereuse pour la mère et le fœtus.
Des pertes vaginales sont normales pendant les premières semaines
suivant l’ablation et peuvent durer pendant un mois. Il s’agit généralement
de pertes de sang lors des premiers jours, de pertes séro-sanguines
d’environ une semaine, puis de pertes abondantes et claires par la
suite. Tout écoulement inhabituel ou nauséabond doit immédiatement
être signalé au médecin. Les autres complications courantes après
l’intervention comprennent des crampes/douleurs pelviennes, des nausées
et des vomissements.
La perforation de l’utérus doit être prise en compte dans le diagnostic
différentiel chez toute patiente se plaignant après l’opération de fortes
douleurs abdominales, de fièvre, d’essoufflements, d’étourdissements,
d’hypotension ou de tout autre symptôme susceptible d’être associé à
une perforation de l’utérus, avec ou sans détérioration des organes de la
cavité abdominale adjacents. Il convient d’inciter les patientes à signaler
immédiatement à leur médecin tout symptôme de ce type.
Préparation des patientes avant le traitement
Le système d’ablation de l’endomètre contrôlée par impédance
NovaSure est conçu pour traiter toute une plage d’épaisseurs
d’endomètre dans la cavité utérine. Il n’est pas nécessaire de réduire
l’épaisseur de la paroi utérine avant l’intervention, qui peut avoir lieu
indifféremment pendant la phase proliférative ou sécrétoire du cycle.
Bien que l’innocuité et l’efficacité du système NovaSure n’aient pas été
entièrement évaluées chez les patientes ayant eu un traitement médical
ou chirurgical préalable, elles ont été évaluées sur un nombre limité de
patientes traitées préalablement par des agonistes de la GnRH, sans
complications ni événements indésirables.
Un saignement actif n’a pas semblé constituer un facteur limitant lors
de l’utilisation du système NovaSure. Il est conseillé d’administrer un
anti-inflammatoire non stéroïdien (AINS) au moins une heure avant le
traitement et de le poursuivre après l’intervention afin de réduire les
crampes utérines peropératoires et post-opératoires.
Mode d’emploi du système d’ablation de l’endomètre
contrôlée par impédance NovaSure
Lire toutes les instructions, les mises en garde et les avertissements
avant utilisation.
1.0 Installation
CONTRÔLEUR RF
NovaSure
DISPOSITIF JETABLE NovaSure
AVEC CORDON DE BRANCHEMENT,
Y COMPRIS DÉSHYDRATANT POUR
TUBULURE D’ASPIRATION
CORDON D’ALIMENTATION
NovaSure
DÉSHYDRATANT POUR TUBULURE
D’ASPIRATION NOVASURE
CARTOUCHE DE CO2 NovaSure PÉDALE NovaSure
1.1 Les éléments suivants sont nécessaires lors de l’utilisation du
système NovaSure:
• un dispositif jetable NovaSure stérile à usage unique ; avec
• cordon de branchement;
• un contrôleur RF NovaSure;
• une pédale NovaSure;
• un cordon d’alimentation secteur NovaSure;
• un déshydratant pour tubulure d’aspiration non stérile NovaSure;
• une cartouche de CO2 NovaSure.
Reniflard
Collier cervical
Rangée
d’électrodes
bipolaires
Poignée avant
Gaine
Poignée
arrière
Tubulure
d’aspiration
Bouton de
déverrouillage
Réglage de la longueur de la cavité
Cannelure de
tubulure de
retour de vide
Cadran WIDTH
(LARGEUR)

11
FRANÇAIS
Remarque: avoir à disposition au moins un autre dispositif jetable,
un autre déshydratant et une autre cartouche de CO2.
1.2 Préparer le contrôleur RF NovaSure. Le placer sur une petite table
à côté de la patiente, dans le champ visuel du chirurgien. Relier le
cordon d’alimentation secteur au contrôleur et le brancher sur la
prise secteur.
1.3 Visser la cartouche de CO2 sur le détendeur au niveau du panneau
arrière du contrôleur jusqu’à ce qu’elle soit serrée.
Interrupteur
basculant
Cartouche de CO2
Cordon
d’alimentation
secteur
1.4 Tourner complètement le bouton du détendeur de CO2 en position
HI (s’il en est équipé).
Remarque: sur les modèles de contrôleurs plus récents, le
détenteur n’est pas doté d’un bouton et l’administration de CO2 est
donc automatiquement régulée. Si votre contrôleur n’est pas équipé
d’un bouton sur le détendeur, passer à l’étape 1.5.
1.5 Appuyer sur l’interrupteur basculant situé sur le panneau arrière du
contrôleur pour le placer en position « on » (Marche).
1.6 Brancher la pédale sur la prise correspondante située sur le
panneau avant du contrôleur.
Remarque: lors du premier allumage du contrôleur RF Modèle
10, l’écran « Sélectionner votre langue » s’affiche. Le réglage par
défaut est l’anglais. Pour sélectionner une autre langue, appuyer
sur le bouton comportant le nom de cette langue. Enregistrer la
sélection en appuyant sur le bouton vert clignotant.
La sélection de la langue est conservée. Pour modifier la sélection de
la langue après la configuration initiale, utiliser l’écran «Paramètres ».
Appuyer sur le nom de la langue pour modifier la langue utilisée sur
l’affichage de l’écran. Pour enregistrer les modifications apportées
aux paramètres, appuyer sur le bouton vert clignotant. Pour annuler
une sélection, appuyer sur le « X » bleu.
2.0 Procédure
2.1 Préparer la patiente pour l’anesthésie.
2.2 Placer la patiente en position gynécologique.
2.3 Procéder à l’anesthésie selon une technique standard.
Prise
2.4 Procéder à un examen bimanuel. Vérifier l’absence d’antéversion ou
de rétroversion prononcée.
2.5 Préparer et couvrir la patiente comme pour la dilatation et le curetage.
2.6 Insérer un spéculum dans le vagin.
2.7 Saisir le col de l’utérus avec un tenaculum.
2.8 Sonder l’utérus afin de mesurer la longueur entre le fond et l’orifice
cervical externe. L’efficacité du système NovaSure n’a pas été
entièrement évaluée chez les patientes ayant une mesure de
l’utérus par sondage supérieure à 10cm.
2.9 Déterminer la longueur du canal cervical et le dilater pour
insérer le dispositif.
Remarque: le diamètre nominal du dispositif jetable NovaSure
est de 6mm.
2.10 Utiliser les mesures de sondage de l’utérus et du canal cervical
pour consulter le tableau de longueur de la cavité (ci-dessous) afin
d’obtenir les paramètres appropriés de longueur de la cavité. Dans
la partie supérieure du tableau, les dimensions ont été modifiées
afin de refléter la longueur des électrodes du dispositif jetable.
Il est important de déterminer correctement la longueur de la cavité
pour garantir un traitement sûr et efficace. Une surestimation de la
longueur de la cavité pourrait provoquer des brûlures au niveau du
canal endocervical.
Avertissement: veiller à ne pas perforer la paroi utérine lors de la
mesure par sondage, de la dilatation ou de l’insertion du dispositif
jetable.
TABLEAU 8. LONGUEUR DE LA CAVITÉ
Sondage de l’utérus (cm)
Longueur du
col de l’utérus
(cm) 10 9,5 9 8,5 8 7,5 7 6,5 6
26,5* 6,5* 6,5* 6,5 6 5,5 5 4,5 4
2,5 6,5* 6,5* 6,5 6 5,5 5 4,5 4
36,5* 6,5 6 5,5 5 4,5 4
3,5 6,5 6 5,5 5 4,5 4
46 5,5 5 4,5 4
4,5 5,5 5 4,5 4
55 4,5 4
5,5 4,5 4
64
* La valeur de 6,5 n’est pas censée refléter la différence numérique entre la longueur du sondage et celle
du canal cervical.
La valeur 6,5 a été entrée, car elle représente la longueur maximale d’extension possible de la rangée
d’électrodes NovaSure.
Contre-indication: ne pas traiter de patiente dont la longueur de
la cavité utérine est inférieure à 4cm, car le canal cervical pourrait
subir des lésions.

12
FRANÇAIS
Remarque: chez les patientes ayant une longueur de cavité utérine
supérieure à 6,0cm, les taux de réussite observés ont été inférieurs
aux taux de réussite globaux de l’étude.
2.11 Ouvrir l’emballage du dispositif jetable NovaSure stérile. Placer
le dispositif jetable muni de son cordon de branchement dans le
champ stérile, tout en veillant à conserver la boîte du déshydratant
pour tubulure d’aspiration non stérile hors du champ stérile.
Avertissement: ne pas utiliser le dispositif jetable stérile à usage
unique si son emballage est endommagé ou si sa stérilité a pu être
compromise.
2.12 Ouvrir la boîte et la pochette du déshydratant pour tubulure
d’aspiration non stérile. Retirer les bouchons rouges.
Mise en garde: le déshydratant pour tubulure d’aspiration est non
stérile et l’emballage ne doit pas être placé dans le champ stérile.
Mise en garde: si le déshydratant pour tubulure d’aspiration est
rose, le remplacer avant de commencer la procédure d’ablation.
2.13 Relier le déshydratant aux cannelures de la tubulure d’aspiration du
dispositif jetable. S’assurer que les cannelures sont complètement
insérées dans la tubulure sur le déshydratant.
2.14 Mise en garde: le dispositif jetable doit se trouver à l’extérieur
de la patiente avant de passer à l’étape 2.15.
2.15 Brancher le cordon du dispositif jetable sur la prise correspondante
située sur le panneau avant du contrôleur.
Prise du dispositif
jetable
Avertissement: le branchement du dispositif jetable NovaSure
sur le contrôleur RF NovaSure lance l’administration de CO2 afin
de purger tout l’air du dispositif jetable et de la tubulure. Cette
opération de purge prend environ 10secondes et doit être effectuée
lorsque le dispositif jetable est à l’extérieur de la patiente. Un
message de purge du dispositif s’affiche sur le modèle 10RFC et
une tonalité pulsée audible retentit tout au long de la procédure
de purge. Lorsque le bip sonore s’arrête et que la DEL s’éteint ou
le message à l’écran disparaît, le dispositif jetable NovaSure peut
êtreinséré en toute sécurité.
Mise en garde: le CO2 s’écoule continuellement à partir du moment
où le dispositif jetable est branché sur le contrôleur jusqu’à ce que le
test d’évaluation de l’intégrité de la cavité utérine de la procédure soit
terminé. Pour réduire la durée d’administration du CO2 et les risques
d’embolie, effectuer la procédure de positionnement immédiatement
après avoir inséré le dispositif jetable et passer directement de la
procédure de positionnement à l’évaluation de l’intégrité de la cavité
utérine.
Avertissement: veiller à ne pas perforer la paroi utérine lors de la
mesure par sondage, de la dilatation ou de l’insertion du dispositif
jetable.
2.16 Déployer le dispositif jetable à l’extérieur du patient et assurez-vous
que le message à l’écran ne s’affiche pas sur le modèle 10RFC
lorsque la matrice est ouverte. Si le message à l’écran s’affiche
toujours sur le modèle 10RFC, fermez et ouvrez à nouveau le
dispositif jetable. Si ceci ne résout pas le problème, remplacer le
dispositif jetable.
2.17 S’assurer que le cadran WIDTH (LARGEUR) indique une largeur
supérieure ou égale à 4,0cm.
Cadran WIDTH
(LARGEUR)
Remarque: si le cadran WIDTH (LARGEUR) indique moins de 4,0cm,
fermer le dispositif jetable et répéter l’étape 2.16 ci-dessus. Si le
cadran WIDTH (LARGEUR) indique toujours moins de 4,0cm, ouvrir un
dispositif jetable neuf et renvoyer le précédent à le Service technique
d’Hologic.
2.18 Déverrouiller le dispositif jetable en enfonçant le bouton de
déverrouillage. Fermer le dispositif jetable en maintenant la poignée
avant fixe et en tirant doucement la poignée arrière vers l’arrière
jusqu’à ce que l’indicateur de rangée fermée, situé au niveau de la
charnière des poignées avant et arrière, indique «ARRAY CLOSED»
(RANGÉE FERMÉE). Ceci indique que la rangée d’électrodes a été
rétractée dans la gaine et que le dispositif jetable est en position
fermée.

13
FRANÇAIS
Indicateur ARRAY CLOSED
(DE RANGÉE FERMÉE)
Bouton de
déverrouillage
2.19 S’assurer que la rangée d’électrodes est entièrement recouverte
par la gaine externe.
2.20 Vérifier que le cadran WIDTH (LARGEUR) indique environ 0,5cm.
2.21 Utiliser la mesure de sondage de l’utérus et les mesures du canal
cervical pour consulter le tableau de longueur de la cavité (ci-dessus)
afin d’obtenir les paramètres appropriés de longueur de la cavité,
comme indiqué à l’étape 2.10 ci-dessus.
Contre-indication: ne pas traiter de patiente dont la longueur de
la cavité utérine est inférieure à 4cm, car le canal cervical pourrait
subir des lésions.
2.22 Utiliser le tableau de longueur de la cavité de l’étape 2.10 afin de
saisir la valeur obtenue pour la longueur au niveau de l’écran de saisie
du contrôleur RF NovaSure en appuyant sur les flèches HAUT/BAS.
2.23 Régler et bloquer le paramètre de la longueur de la cavité du
dispositif jetable sur la valeur obtenue ci-dessus. (Voir l’étape 2.21.)
S’assurer que le collier cervical est complètement rétracté en
position proximale.
2.24 Confirmez que le col de l’utérus est dilaté à un minimum de 6mm
(le diamètre nominal du dispositif jetable NovaSure).
2.25 Maintenir une légère traction sur le tenaculum pour réduire au
maximum l’angle de l’utérus.
2.26 Aligner le dispositif jetable sur l’axe de l’utérus lors de son insertion
dans la cavité utérine au travers du col de l’utérus. Faire progresser
le dispositif jetable en le tenant par la poignée avant jusqu’à ce que
l’extrémité distale de la gaine touche le fond.
#10
Avertissement: si le dispositif jetable est difficile à insérer dans le
canal cervical, utiliser son jugement clinique pour déterminer si une
dilatation plus poussée est nécessaire.
2.27 Retirer le dispositif jetable d’environ 0,5cm du fond. Presser
lentement les poignées (NE PAS VERROUILLER) jusqu’à sentir
uneaugmentation de la résistance.
Le cadran WIDTH (LARGEUR) doit indiquer environ 0,5cm.
Àcestade, la gaine externe a été rétractée.
0,5 cm

14
FRANÇAIS
2.28.Continuer à presser lentement ensemble les poignées du dispositif
jetable tout en observant un léger mouvement de va-et-vient du
dispositif jetable sur environ 0,5cm par rapport au fond et en
faisant pivoter la poignée du dispositif jetable de 45° dans le sens
inverse des aiguilles d’une montre à partir du plan vertical et de
45° dans le sens des aiguilles d’une montre à partir du plan vertical
jusqu’au verrouillage des poignées.
Le cadran WIDTH (LARGEUR) doit indiquer une largeur supérieure
à2,5cm.
Remarque: une fois que les poignées du dispositif jetable sont
verrouillées, l’utérus doit se déplacer avec le dispositif jetable.
2.29 Déplacer délicatement le dispositif jetable au moyen de mouvements
antérieurs, postérieurs et latéraux.
2.30 Pour terminer le positionnement, retirer légèrement le dispositif
jetable jusqu’à ce que la mesure du cadran WIDTH (LARGEUR)
redescende de 0,2–0,5 cm environ.
2.31 Maintenir le tenaculum et avancer le dispositif jetable lentement
et délicatement jusqu’au fond. Le cadran WIDTH (LARGEUR) doit
indiquer une largeur supérieure ou égale à la mesure précédente.
2.32 Faire glisser le collier cervical vers l’avant en appliquant une légère
pression sur la languette du collier cervical, jusqu’à ce qu’il forme
un joint contre l’orifice cervical externe.
2.33 Lire la distance entre les cornes (2,5 cm minimum) sur le cadran
WIDTH (LARGEUR).
Contre-indication: ne pas traiter de patiente dont la cavité utérine
mesure moins de 2,5cm de large, telle que déterminée par le
cadran WIDTH (LARGEUR) du dispositif jetable suite au déploiement
du dispositif.
Mise en garde: si la notification ARRAY POSITION (POSITION
DE L’ÉLECTRODE) apparaît, consulter la section Résolution des
problèmes sous « DEL ARRAY POSITION (POSITION DE L’ÉLECTRODE)
allumée/Alarme POSITION DE L’ÉLECTRODE) » selon le modèle du
contrôleur.
2.34 Saisir la valeur indiquée sur le cadran WIDTH (LARGEUR) au niveau
de l’écran de saisie du contrôleur RF NovaSure en appuyant sur les
flèches HAUT/BAS.
2.35 Le système peut fonctionner soit en mode automatique, soit en
mode manuel. En mode automatique, le cycle d’ablation démarre
automatiquement après la fin d’un test d’évaluation de l’intégrité
de la cavité utérine réussi. En mode manuel, le cycle d’ablation ne
démarre pas automatiquement après la fin d’un test d’évaluation
de l’intégrité de la cavité utérine réussi.
Légère pression
Pression ferme

15
FRANÇAIS
Remarque: le placement correct de la rangée d’électrodes contre le fond est important pour un traitement sûr et efficace. Si une partie de
la rangée d’électrodes ou le bord distal de la gaine externe est positionné dans le canal endocervical en cours de traitement, il existe un
risque accru de brûlure endocervicale.
Fond
Rangée
d’électrodes
Bord de la
gaine
Canal endocervical
Le bord de la gaine se trouve dans
le segment inférieur de l’utérus
Rangée
d’électrodes
Canal endocervical Bord de la
gaine
Le bord de la gaine se trouve
dans le canal endocervical
Fond
POSITIONNEMENT INCORRECT POSITIONNEMENT CORRECT

16
FRANÇAIS
Remarque: une fuite de CO2 peut se produire au niveau de l’orifice
cervical externe en raison d’une dilatation trop importante du col de
l’utérus. Des bulles visibles ou un «sifflement» de gaz qui s’échappe
peuvent accompagner la fuite de CO2 dans ces cas-là.
C. Si l’évaluation de l’intégrité de la cavité utérine échoue après des
tentatives raisonnables d’exécution des procédures de résolution
des problèmes (étape 2.36), interrompre l’intervention.
Remarque: le retrait du dispositif jetable de la cavité utérine,
après avoir terminé l’évaluation de l’intégrité de la cavité utérine,
nécessite un test d’évaluation de l’intégrité de la cavité utérine
supplémentaire lors de la réinsertion du dispositif jetable (que le
test d’évaluation précédent ait réussi ou non) avant de pouvoir
procéder à l’ablation.
2.37 Mode manuel uniquement
Lorsque le système fonctionne en mode manuel, le cycle d’ablation
ne démarre pas automatiquement après un test d’évaluation
de l’intégrité de la cavité utérine réussi. Une fois qu’un test
d’évaluation de l’intégrité de la cavité utérine réussi a été terminé,
appuyer sur le bouton ACTIVER et appuyer une deuxième fois sur la
pédale pour
lancer le cycle d’ablation.
Remarque : sur tous les contrôleurs RF Modèle 10, une vérification
préalable du vide se fait automatiquement avant de commencer le
cycle d’ablation. L’écran « Vérification du vide en cours... » apparaît
et un bip sonore retentit pendant 10 secondes au plus pendant la
vérification préalable du vide.
Au cours du cycle d’ablation, un écran « RF ACTIVÉE » indiquant la
durée totale permet de suivre la durée de l’ablation.
Remarque: l’administration de puissance RF peut être interrompue
à tout moment en appuyant sur la pédale.
2.38 Après l’arrêt automatique du cycle d’ablation (environ 90 secondes),
rétracter complètement le collier cervical jusqu’à sa position
proximale en utilisant la languette située sur le collier cervical.
Mise en garde: le collier cervical doit être complètement rétracté
jusqu’à sa position proximale de manière à réduire au maximum le
risque de détérioration de la gaine lors de la fermeture de la rangée
d’électrodes.
Fonctionnement du contrôleur RF Modèle 10
A. Mode automatique
Pour faire fonctionner le contrôleur RF Modèle 10 en mode automatique,
appuyer sur le bouton « Changer mode » lorsque celui-ci apparaît au bas de
l’écran. Passer à l’étape 2.36, mais ne pas suivre l’étape 2.37 si le système
fonctionne en mode automatique.
B. Mode manuel
Remarque: le mode manuel est le mode de fonctionnement par
défaut du système.
Pour faire fonctionner le système en mode manuel, ne pas appuyer sur
le bouton « Changer mode » avant de lancer le test d’évaluation de
l’intégrité de la cavité utérine. Suivre les étapes 2.36 et 2.37.
2.36 Lancer la procédure du test d’évaluation de l’intégrité de la cavité utérine
en appuyant une fois sur la pédale. « Évaluation de la cavité en cours... »
s’affiche sur l’écran alors que cinq points s’éteignent et s’allument de
manière séquentielle. La durée du test est d’environ 7à30secondes.
L’écran « Évaluation de la cavité terminée... » apparaît une fois le
test d’évaluation de l’intégrité de la cavité utérine réussi et lorsque le
système peut administrer de l’énergie RF. La puissance ne peut pas être
appliquée au dispositif jetable tant que l’écran « Évaluation de la cavité
terminée... » n’est pas affiché.
Si le test d’évaluation de l’intégrité de la cavité utérine échoue,
l’écran affiche « Échec évaluation cavité » avec les étapes de
résolution des problèmes à suivre.
A. En cas de suspicion de perforation utérine, l’intervention doit être
immédiatement interrompue.
B. Si le test d’évaluation de l’intégrité de la cavité utérine échoue à
nouveau, rechercher la présence d’une fuite dans le système ainsi
qu’entre le col de l’utérus et le collier cervical. Vérifier tous les
raccords de tubulure et s’assurer qu’un déshydratant pour tubulure
d’aspiration a été installé. Si la fuite semble se trouver au niveau
du col de l’utérus et ne peut pas être résolue à l’aide du collier
cervical, utiliser un autre tenaculum pour saisir le col de l’utérus
autour de la gaine. Répéter le test d’évaluation de l’intégrité de la
cavité utérine en appuyant sur la pédale.

17
FRANÇAIS
Collier
cervical
À la fin du cycle d’ablation, l’écran « Procédure terminée » s’affiche avec
un résumé de l’intervention. L’écran « Procédure terminée » capture les
informations suivantes pour chaque intervention :
• longueur de la cavité ;
• largeur de la cavité ;
• puissance ;
• durée d’ablation RF.
2.39 Déverrouiller le dispositif jetable en enfonçant le bouton de
déverrouillage. Fermer le dispositif jetable en maintenant la poignée
avant fixe et en tirant doucement la poignée arrière vers l’arrière,
jusqu’à ce que l’indicateur de rangée fermée, situé au niveau de la
charnière des poignées avant et arrière, indique «ARRAY CLOSED»
(RANGÉE FERMÉE). Ceci indique que la rangée d’électrodes a été
rétractée dans la gaine et que le dispositif jetable est en position
fermée.
Remarque: s’il est difficile de fermer et de retirer le dispositif
jetable, voir la section Résolution des problèmes, «Difficulté à
fermer et à retirer le dispositif jetable après l’ablation».
Mise en garde: pour éviter d’endommager le dispositif, procéder
en douceur lors du retrait de la rangée d’électrodes.
2.40 Retirer le dispositif jetable de la patiente.
2.41 ÉTEINDRE LE CONTRÔLEUR RF NOVASURE.
2.42 Procéder aux soins postopératoires selon les procédures standard.
2.43 Laisser la patiente sortir de l’hôpital ou du cabinet médical comme
indiqué par le médecin responsable.
Maintenance périodique et entretien
Le contrôleur RF a été conçu et testé conformément à la norme CEI
60601-1 et aux autres normes de sécurité. Aucune maintenance n’est
nécessaire car le système exécute des auto-vérifications lors de la mise
sous tension. Pour nettoyer le contrôleur, reportez-vous à la section
«Nettoyage et désinfection».
La durée de vie prévue du contrôleur RF est de cinq ans à condition que
les dommages causés par un impact physique, comme une chute ou
une manipulation brutale soient évités. Si le contrôleur tombe ou subit
un impact physique grave, cessez de l’utiliser et contactez le service
technique Hologic. Reportez-vous à la section «Service technique et
informations sur le retour des produits».
Laisser la patiente sortir de l’hôpital ou du cabinet médical comme
indiqué par le médecin responsable.
Avertissement : aucune modification de cet appareil n’est autorisée.
Test de puissance de sortie RF
Le contrôleur RF NovaSure Modèle 10 comporte un test de puissance
de sortie automatique intégré à l’autotest à la mise sous tension
(POST). Pendant le POST, l’émission de puissance (Pc) du contrôleur est
administrée à une résistance de dérivation (Rs) se trouvant à l’intérieur
du contrôleur. La Pc doit être de 180 watts et la Rs nominale de 25 ohms.
Pendant le POST, aucune puissance n’est délivrée au connecteur du
dispositif jetable à l’avant du contrôleur.
Le contrôleur RF NovaSure Modèle 10 procède au POST
automatiquement à la mise sous tension. Pour consulter les informations
sur le POST, accéder à Paramètres et défiler jusqu’à Infos système.
Appuyer sur le bouton « Afficher info ».
Remarque: en cas de défaillance du système pendant le POST,
mettre le module d’entrée de l’alimentation hors service et
recommencer le POST. En cas de deuxième défaillance du système,
mettre le contrôleur RF hors Service technique. Service technique
d’Hologic.
Mise en garde: ne pas essayer de réparer le contrôleur en cas de
suspicion de problèmes. Suivre le guide de résolution des problèmes
de ce manuel. Si les problèmes persistent, appeler l’assistance
technique d’Hologic pour obtenir des instructions.
Dispositif jetable NovaSurestérile : aucune maintenance n’est
nécessaire. À usage unique exclusivement. Ne pas réutiliser ou
restériliser le dispositif jetable NovaSure.

18
FRANÇAIS
Icônes de l’écran du contrôleur RF NovaSure Modèle 10
Ci-après figure une description des icônes se trouvant sur l’écran du
contrôleur RF NovaSure Modèle 10.
Icône Paramètres :
Appuyer sur ce bouton pour afficher
les options des paramètres pour la
langue, la luminosité et le volume.
Icône Dernière intervention :
Appuyer sur ce bouton pour
afficher l’écran « Procédure
terminée » et passer en revue
le résumé de la dernière
intervention.
Icône Aide :
Appuyer sur ce bouton pour afficher des
informations supplémentaires relatives à
l’étape de l’intervention en cours. Cette icône
affiche une version abrégée de la langue du
mode d’emploi.
Remarque: lorsque l’on appuie sur l’icône « Dernière
intervention », seule l’intervention précédente est affichée. Les
informations relatives aux interventions antérieures à l’intervention
la plus récente ne seront pas disponibles.
Remarque: dans l’écran « Paramètres », appuyer sur les boutons
« - » ou « + » pour régler le volume et la luminosité.
Remarque: lors du premier allumage du contrôleur RF Modèle
10, l’écran « Sélectionner votre langue » s’affiche. Le réglage par
défaut est l’anglais. Pour sélectionner une autre langue, appuyer
sur le bouton comportant le nom de cette langue. Enregistrer la
sélection en appuyant sur le bouton vert clignotant. La sélection
de la langue est conservée. Pourmodifier la sélection de la langue
après la configuration initiale, utiliser l’écran « Paramètres ».
Appuyer sur le nom de la langue pour modifier la langue utilisée sur
l’affichage de l’écran. Pour enregistrer les modifications apportées
aux paramètres, appuyer sur le bouton vert clignotant. Pourannuler
une sélection, appuyer sur le « X » bleu.
Résolution des alarmes les plus courantes
ALARME DE L’ÉVALUATION DE L’INTÉGRITÉ DE LA CAVITÉ
UTÉRINE
Si le test d’évaluation de l’intégrité de la cavité utérine échoue, l’écran
affiche « Échec évaluation cavité » avec une version abrégée des astuces
de résolution des problèmes ci-dessous. L’échec du test d’évaluation de
l’intégrité de la cavité utérine est dû à l’impossibilité de mettre la cavité
sous pression qui peut résulter :
1. D’une fuite au niveau du dispositif: vérifier que le filtre déshydratant
pour tubulure d’aspiration a été installé. Vérifier tous les raccords
des tubulures pour s’assurer que les connexions sont étanches.
2. D’une fuite au niveau de l’orifice cervical externe: rechercher des
bulles visibles ou un «sifflement» au niveau de l’orifice cervical
externe.
Utiliser la languette située sur le collier cervical pour faire avancer le
collier cervical vers l’orifice cervical externe pour assurer une bonne
étanchéité. Procéder de nouveau au test d’évaluation de l’intégrité
de la cavité utérine. Si le test d’évaluation de l’intégrité de la cavité
utérine échoue à nouveau, utiliser un second tenaculum pour saisir
le col de l’utérus autour de la gaine du dispositif jetable NovaSure.
Procéder de nouveau au test d’évaluation de l’intégrité de la cavité
utérine.
3. D’une perforation de l’utérus: en cas de suspicion de perforation
utérine, l’intervention doit être immédiatement interrompue.
Remarque: une fuite de CO2 peut se produire au niveau de l’orifice
cervical externe en raison d’une dilatation trop importante du
col de l’utérus. Des bulles visibles ou un «sifflement» de gaz qui
s’échappe peuvent accompagner la fuite de CO2 dans ces cas-là.
Remarque: lors de l’exécution des étapes de résolution des
problèmes sur le contrôleur RF Modèle 10, appuyer sur le bouton
«?» à l’écran et utiliser les boutons de défilement de droite pour
deplus amples informations. Pour revenir à l’écran principal à
partir des autres astuces de résolution des problèmes, appuyer
surle « X » en haut à droite de l’écran.
Si l’évaluation de l’intégrité de la cavité utérine échoue après des
tentatives raisonnables d’exécution de la procédure de résolution des
problèmes (étape 2.36), interrompre l’intervention.
ALARME DE VIDE
L’alarme de vide se produit lorsque le niveau de vide est en dehors de sa
plage spécifiée. Ceci peut résulter d’une ou de plusieurs des conditions
suivantes:
• un col de l’utérus trop dilaté;
• un mauvais contact entre le collier cervical et l’orifice cervical externe;
• le reniflard est en position fermée;
• une obstruction du ou des filtres (deux) du dispositif jetable ou du
déshydratant; ou
• une obstruction dans le dispositif jetable.
Si la vérification du vide échoue, l’écran affiche « Échec du vide » avec une
version abrégée des astuces de résolution des problèmes suivantes :

19
FRANÇAIS
• Enfoncer doucement un dilatateur pour utérus de 2 à 3,5 mm ou une
sonde à l’intérieur du reniflard.
• Vérifier la position du collier cervical et le repositionner si besoin est.
Utiliser la languette située sur le collier cervical pour faire avancer
le collier cervical vers l’orifice cervical externe pour assurer une
bonne étanchéité. Vérifier que de l’air n’est pas aspiré par le col de
l’utérus en raison d’une fuite entre le collier cervical et l’entrée du
canal cervical. Side l’air est aspiré par le canal cervical, essayer de
repositionner le collier cervical et la tige du dispositif jetable pour
remédier au problème.
• S’assurer que la cartouche d’aspiration située sur le dispositif jetable
est verticale et que la tubulure du dispositif n’est pas enroulée autour
de la jambe de la patiente.
• Vérifier tous les raccords des tubulures pour s’assurer que les
connexions sont étanches. Vérifier les connecteurs de tubulure
à pression au niveau du tube de déshydratant. Remplacer le
déshydratant s’il est rose. S’assurer que le filtre se trouvant à côté de
la connexion jetable sur la tubulure de retour de vide est serré.
• Retenter l’ablation.
Si l’écran « Échec du vide » s’affiche à nouveau:
• Débrancher le dispositif jetable du contrôleur RF.
• Retirez le dispositif jetable et remplacez-le par un nouveau.
• Tenter à nouveau l’ablation avec le dispositif neuf.
Remarque: lors de l’exécution des étapes de résolution des
problèmes sur le contrôleur RF Modèle 10, appuyer sur le bouton
«? » à l’écran et utiliser les boutons de défilement de droite pour de
plus amples informations. Pour revenir à l’écran principal à partir
des autres astuces de résolution des problèmes, appuyer sur le
« X» en haut à droite de l’écran.
Si l’alarme du vide se déclenche avec le nouveau dispositif, annuler la
procédure.
Remarque: le retrait du dispositif jetable de la cavité utérine,
après avoir terminé l’évaluation de l’intégrité de la cavité utérine,
nécessite un test d’évaluation de l’intégrité de la cavité utérine
supplémentaire lors de la réinsertion du dispositif jetable (que le
test d’évaluation précédent ait réussi ou non) avant de pouvoir
procéder à l’ablation.
Cartouche de CO2 presque vide ou vide
Un écran indique « Remplacer la cartouche de CO2 » avec une image
de l’arrière du contrôleur. Un bip sonore est généré à une fréquence
d’une tonalité par seconde. Les messages d’alarme présents avant
l’alarme restent identiques lorsque la cartouche de CO2 est remplacée.
L’activation de la pédale ne coupe pas l’alarme sonore.
1. Remplacer la cartouche de CO2 pour couper le bip sonore.
Remarque: il n’est pas nécessaire de retirer le dispositif jetable de
la patiente avant de remplacer la cartouche.
2. Poursuivre l’intervention.
Alarme de POSITION DE L’ÉLECTRODE
Le message Position de l’électrode s’affiche lorsque la rangée
d’électrodes n’est pas entièrement ouverte. Le contrôleur ne peut
pas procéder à l’ablation lorsque le message Position de l’électrode
s’affiche. Si l’alarme de POSITION DE L’ÉLECTRODE se produit, l’écran
affiche «Vérifier l’électrode » avec une version abrégée des astuces de
résolution des problèmes suivantes :
1. Déplacer délicatement l’extrémité proximale du dispositif jetable
et regarder si le message Position de l’électrode ne s’affiche plus.
S’ilest toujours affiché, procéder comme suit:
2. Essayer de repositionner délicatement le dispositif jetable NovaSure:
A. Rétracter partiellement la rangée d’électrodes dans la gaine
en relâchant le bouton de déverrouillage de la poignée du
dispositif jetable ;
B. Retirer légèrement du fond le dispositif jetable ;
C. Redéployer lentement la rangée d’électrodes du dispositif
jetable tout en le balançant délicatement dans un mouvement
d’avant en arrière et en verrouillant ses poignées; et
D. Repositionner le dispositif jetable contre le fond selon la
procédure de positionnement décrite aux étapes 2.26 à 2.33.
3. En cas de rétroversion de l’utérus, veiller tout spécialement à éviter
toute perforation. Appliquer une légère traction caudale sur le col
de l’utérus avec le tenaculum et soulever la poignée du dispositif
jetable vers le plafond (dans l’axe de l’utérus) tout en procédant au
positionnement.
4. Si le message Position de l’électrode est toujours affiché, rétracter
entièrement la rangée d’électrodes du dispositif jetable et retirer ce
dernier de la patiente.
5. Déployer le dispositif jetable en dehors du corps de la patiente;
s’assurer que la rangée d’électrodes n’est pas endommagée et que
le message Position de l’électrode ne s’affiche plus.
6. Tenter de réinsérer, redéployer et repositionner le dispositif jetable
selon la procédure de positionnement décrite à la section2.0.
7. Si le message Position de l’électrode est toujours affiché, remplacer
par un dispositif jetable neuf.
8. Si le message Position de l’électrode s’affiche avec un dispositif
jetable neuf, interrompre la procédure.
Remarque: lors de l’exécution des étapes de résolution des
problèmes sur le contrôleur RF Modèle 10, appuyer sur le bouton
« ? » à l’écran et utiliser les boutons de défilement de droite pour de
plus amples informations. Pour revenir à l’écran principal à partir
des autres astuces de résolution des problèmes, appuyer sur le
« X » en haut à droite de l’écran.
Veuillez passer à la page suivante pour
le reste du mode d’emploi. Dépannage
supplémentaire.

20
FRANÇAIS
Perforation de l’utérus suspectée
Avant l’application d’énergie Pendant ou après l’application
d’énergie:
1. Interrompre l’intervention. 1. Interrompre l’intervention.
2. S’assurer de la stabilité de la
patiente. 2. S’assurer de la stabilité de la
patiente.
3. Envisager un examen pour
détecter la perforation. 3. Vérifier l’absence de lésions
viscérales.
4. Reprogrammer l’intervention, le
cas échéant. 4. Reprogrammer l’intervention, le
cas échéant.
La rangée d’électrodes ne se déploie pas complètement et ne se
verrouille pas dans l’utérus
1. Rétracter partiellement la rangée d’électrodes dans la gaine
(maintenir la poignée avant fixe et tirer la poignée arrière en
l’éloignant de la patiente).
2. Repositionner le dispositif jetable dans la cavité.
3. Redéployer la rangée d’électrodes dans la cavité.
4. Si le dispositif jetable ne se verrouille pas, le retirer de l’utérus.
5. Examiner le dispositif jetable pour voir s’il n’est pas endommagé.
6. Essayer d’ouvrir le dispositif jetable et de le verrouiller en dehors de
la patiente.
7. S’il est endommagé, remplacer le dispositif jetable.
8. Si le dispositif jetable n’est pas endommagé, le réinsérer dans la
cavité utérine de la patiente et essayer de procéder audéploiement.
9. S’il est impossible de déployer le dispositif jetable à une distance
minimale entre les cornes de 2,5 cm, interrompre l’intervention.
10. Envisager une perforation de l’utérus comme une cause possible du
non-déploiement.
Difficulté à fermer et à retirer le dispositif jetable après
l’ablation
Confirmer que le bouton de déverrouillage est enfoncé:
• Si c’est le cas, retirer progressivement le dispositif jetable de
lapatiente.
• Sinon, appuyer sur le bouton de déverrouillage et retenter de
fermer le dispositif jetable. S’il est encore difficile à fermer, retirer
progressivement le dispositif jetable de la patiente.
4. La DEL ARRAY POSITION (POSITION DE L’ÉLECTRODE) n’est pas
allumée.
L’écran «Procédure terminée» n’apparaît pas sur le modèle 10
RFC à la fin d’une procédure.
Si l’alimentation n’a pas été appliquée pendant au moins 30 secondes,
l’écran «Procédure terminée» n’apparaîtra pas sur le modèle 10RFC.
Procédure non terminée
1. Retirez l’appareil du patient et déployez la matrice
a. Vérifiez que la matrice n’est PAS endommagée
b. Vérifiez que la position de la matrice ne s’affiche PAS
2. Pour plus d’aide, appuyez sur ?
Si a et b sont confirmés, réinsérez le dispositif et APPUYEZ SUR
L’INTERRUPTEUR AU PIED pour réessayer le traitement.
Si un problème est détecté, remplacez le dispositif et redémarrez
la procédure.
1. Retirer le dispositif jetable NovaSure de l’utérus après avoir rétracté
entièrement sa rangée d’électrodes dans la gaine:
A. Relâcher le bouton de déverrouillage du dispositif jetable;
B. Maintenir la poignée avant du dispositif jetable fixe;
C. Tirer la poignée arrière du dispositif jetable vers l’arrière.
2. Examiner le dispositif jetable pour voir s’il est endommagé. Déployez
entièrement la matrice d’électrodes à l’extérieur du patient,
démontrant que le message ne s’affiche pas sur le modèle 10 RFC.
3. Si le dispositif jetable n’est pas endommagé et que l’écran de
message n’apparaît pas sur le modèle 10 RFC, réinsérer, redéployer et
réessayer le traitement.
4. Si le problème persiste, remplacer le dispositif jetable par un neuf.
5. Retenter l’intervention. Si le problème persiste, interrompre
l’intervention.
L’écran «RF ACTIVÉ» n’apparaîtra pas sur le modèle 10 RFC
1. Si le contrôleur RF NovaSure est branché et sous tension, si le
bouton ENABLE (ACTIVER) a été appuyé et que la puissance n’est
pas délivrée par le contrôleur lorsque la pédale est actionnée,
vérifier le branchement de celle-ci. S’assurer également que le test
d’ÉVALUATION DE L’INTÉGRITÉ DE LA CAVITÉ UTÉRINE a réussi.
2. Si le problème persiste, interrompre l’intervention.
Les valeurs HAUT/BAS n’apparaissent pas lorsque les boutons
appropriés sont appuyés
S’assurer que le dispositif jetable est relié au contrôleur. Les valeurs
n’apparaissent que si le dispositif jetable est correctement branché
surle contrôleur.
Instructions de remplacement
Le contrôleur RF NovaSure utilise deux fusibles situés sur un porte-fusibles
dans le module d’entrée de l’alimentation. Les fusibles utilisés sont de
type T5AH, 250 V. Pour accéder au module, il suffit de soulever le volet
du porte-fusibles avec un tournevis plat. Si nécessaire, il est possible
de retirer le porte-fusibles et de changer les fusibles. Le remontage se
fait en suivant ces étapes dans le sens inverse. Tout produit NovaSure
potentiellement défectueux doit être renvoyé à Hologic pour être évalué.
Suivre les instructions figurant à la fin de ce manuel, dans la section
Renvois au service après-vente, pour obtenir un numéro d’autorisation de
renvoi de matériel (N° RMA). Ne pas jeter le dispositif jetable NovaSure.

21
FRANÇAIS
Spécifications techniques
Dispositif jetable NovaSure
1. Le dispositif jetable NovaSure ne contient pas de latex.
2. Le dispositif jetable NovaSure est un dispositif de classe III
conformément à la réglementation de la FDA.
3. Le dispositif jetable NovaSure est un dispositif de classe IIB
conformément à la directive 93/42/CEE relative aux dispositifs
médicaux.
4. Dimensions hors tout du dispositif jetable NovaSure :
48,3 cm x 15,2 cm x 5 cm (19 po x 6 po x 12 po).
5. La tension nominale du dispositif jetable NovaSure est de 153 V.
Contrôleur RF NovaSure
1. Le contrôleur RF NovaSure peut être utilisé avec des prises de 100 à
240 V c.a. et consomme 5 A au maximum.
2. Le contrôleur RF NovaSure est un appareil de type BF résistant aux
défibrillations de classe I, conformément à la norme CEI 60601-1.
3. Le contrôleur RF NovaSure est un dispositif de classe III
conformément à la réglementation de la FDA.
4. Le contrôleur RF NovaSure est un dispositif de classe IIB selon la
directive 93/42/CEE relative aux dispositifs médicaux.
5. Le contrôleur RF a satisfait aux essais de conformité concernant
les restrictions imposées aux dispositifs médicaux conformément
à la norme CEI 60601-1-2 ÉD.4.0: 2014. Ces limites sont conçues
pour fournir une protection raisonnable contre les interférences
nuisibles dans une installation médicale type. Cet appareil produit,
utilise et peut émettre de l’énergie de radiofréquence et s’il n’est pas
installé et utilisé conformément aux instructions, il peut provoquer
des interférences nuisibles aux autres appareils situés à proximité.
Il n’existe toutefois aucune garantie que des interférences ne se
produiront pas dans une installation particulière. Si cet appareil
provoque des interférences nuisibles pour d’autres appareils, ce
qui peut être déterminé en allumant et en éteignant l’appareil, il est
conseillé àl’utilisateur d’essayer de corriger les interférences à l’aide
d’une ou de plusieurs des mesures suivantes:
• réorienter ou déplacer l’appareil récepteur ;
• augmenter la distance entre les appareils ;
• brancher l’appareil sur une prise reliée à un circuit différent de celui
du ou des autres appareils ;
• contacter l’assistance technique d’Hologic (ou le fabricant de l’autre
appareil) pour demander une assistance.
6. Le contrôleur répond aux exigences des normes CEI 60601-1/
UL60601-1, CEI 60601-2-2 et CSA C22.2 Nº 601.1.
7. Le contrôleur doit être expédié uniquement dans son emballage
Hologic d’origine. Les conditions environnementales d’utilisation,
d’expédition et de stockage requises sont indiquées ci-dessous.
8. La tension de crête maximale absolue produite par le contrôleur RF
NovaSure est de 153volts. Les accessoires utilisés avec le contrôleur
RF doivent avoir une tension nominale supérieure ou égaleà 153 volts.
9. La puissance de crête maximale absolue produite par le contrôleur
RF NovaSure est de 216watts.
10. Poids du contrôleur RF NovaSure: 11 kg, sans son emballage.
11. Hauteur : 32 cm ; largeur : 19 cm ; profondeur : 35,5 cm
(12,5 po ; 7,5 po ; 14,5 po).
12. La pression maximale de CO2 administrée par le contrôleur RF
NovaSure et le dispositif jetable NovaSure doit être de 90 ± 10mmHg.
Le débit maximal de CO2 produit par le contrôleur RF NovaSure relié
au dispositif jetable NovaSure doit être de 95 ±15ml/min. (Le débit
maximal de CO2 produit par le contrôleur RF NovaSuresans dispositif
jetable NovaSure relié est de 105 - 130ml/min.)
13. Le générateur RF Novasure doit être utilisé sans électrode neutre.
Puissance contre résistance
Puissance mesurée (watts)
Résistance de charge (ohms)
Puissance contre résistance
Puissance mesurée (watts)
Résistance de charge (ohms)

22
FRANÇAIS
Directives de sécurité électromagnétique
Tableau 1 - Recommandations et déclaration du fabricant –
Émissions électromagnétiques et immunité électromagnétique
Recommandations et déclaration du fabricant – Émissions
électromagnétiques
Le contrôleur RF NovaSure est conçu pour fonctionner dans l’environnement
électromagnétique précisé ci-dessous. Le client ou l’utilisateur du contrôleur RF
NovaSure doit s’assurer qu’il est utilisé dans cet environnement.
Test
d’émissions Conformité Environnement
électromagnétique — Directives
Émissions RF
CISPR 11
Groupe 1 Le contrôleur RF NovaSure
doit émettre de l’énergie
électromagnétique afin de remplir
la fonction pour laquelle il a été
conçu. L’équipement électronique à
proximité peut être affecté.
Émissions RF
CISPR 11
Classe A Le contrôleur RF NovaSure est
conçu pour être utilisé dans les
établissements de soins de santé
professionnels, y compris les
hôpitaux et les cabinets médicaux.
Avertissement : conformément à
ses caractéristiques d’ÉMISSIONS,
cet appareil convient à une
utilisation dans les zones
industrielles et les hôpitaux
(CISPR 11 Classe A). S’il est
utilisé dans un environnement
résidentiel (pour lequel la
catégorie CISPR 11 Classe B
est normalement requise) cet
appareil peut ne pas offrir
une protection adéquate aux
services de communication par
radiofréquence. Il sera peut
être nécessaire à l’utilisateur
de prendre des mesures
d’atténuation, comme le
déplacement ou la réorientation
de l’appareil.
Émissions
harmoniques
CEI 61000-3-2
Classe A
Fluctuations
de tension/
papillotement
conformément
à la norme
CEI 61000-3-3
Conforme
Avertissement: dans certaines circonstances, l’utilisation d’un
dispositif haute fréquence entraîne un risque de brûlures sur
d’autres sites. Éviter le contact peau à peau en insérant par
exemple de la gaze sèche.
Avertissement: un potentiel de décharge électrostatique existe avec
tout dispositif électrochirurgical, et une stimulation neuromusculaire
peut se produire. Lorsque ce dispositif est correctement utilisé dans
l’utérus, le risque de stimulation musculaire, particulièrement du
muscle cardiaque, est minime.
Conditions environnementales
Contrôleur RF NovaSure
Conditions de fonctionnement, hors emballage
Altitude 0 à 3030 m (0 à 10 000 pieds)
Température 10°C à 40°C (50 °F à 104 °F)
Humidité 15 à 85% HR (sans condensation)
Conditions hors fonctionnement, sous emballage
Altitude 0 à 12 120 m (0 à 40 000 pieds)
Température –30°C à 60°C (–22 °F à 140 °F)
Humidité 85% HR, (sans condensation)
Jusqu’à 90% HR, (sans condensation)
Performances importantes Caractéristiques
• L’air doit être purgé pendant 10 secondes avant l’insertion chez le
patient.
• L’évaluation de l’intégrité de la cavité (CIA) doit mesurer une
pression de 50 ± 10 mmHg pendant 3 secondes minimum pour
être réussie. Sinon, la CIA signalera une erreur. Le contrôleur RF
n’autorisera pas l’ablation tant que la CIA ne sera pas réussie.
• Puissance RF : La gamme de puissance RF délivrée est de 55 à
180 watts (+/- 20 %).
• Surveillance de la pression à vide : Pendant une ablation, la
pression à vide doit être comprise entre 17,78 ± 5,08 mmHg et
152,4 ± 25,4 mmHg. Si la pression à vide dépasse cette plage, le
contrôleur met fin à l’ablation.
• Surveillance de l’impédance : Le contrôleur RF met fin à une
ablation lorsque l’impédance tissulaire mesurée atteint 50 ohms.
• Minuterie de deux minutes : Après deux minutes d’énergie RF, le
contrôleur met fin à l’ablation.
• Délai d’attente de dix minutes : une fois la procédure d’ablation
terminée, le contrôleur se met en attente pendant 10 minutes,
pendant lesquelles le contrôleur n’est pas en mesure de fournir de
l’énergie.
• Protection contre les courts-circuits DC: Si le contrôleur RF détecte
un court-circuit (c.-à-d. <13 +/-6ohms), l’ablation prendra fin.

23
FRANÇAIS
Tableau 2 - Recommandations et déclaration du fabricant –
Immunité électromagnétique
Recommandations et déclaration du fabricant – Immunité
électromagnétique
Le contrôleur RF NovaSure est conçu pour fonctionner dans l’environnement
électromagnétique précisé ci-dessous. Le client ou l’utilisateur du contrôleur RF
NovaSure doit s’assurer qu’il est utilisé dans cet environnement.
Test
d’immunité CEI 60601
Niveau d’essai Conformité
Niveau
Environnement électro-
magnétique – Recom-
mandations
Décharge
électrosta-
tique (DES)
CEI 61000-
4-2
± 2 kV, ± 4 kV,
± 8 kV au
contact
± 2 kV, ± 4 kV,
± 8 kV au
contact
Les sols doivent être
en bois, en béton ou
en carrelage. S’ils sont
recouverts d’un matériau
synthétique, l’humidité
relative doit être d’au
moins 30 %.
± 2 kV, ± 4 kV,
± 8 kV, ± 15 kV
dans l’air
± 2 kV, ± 4 kV,
± 8 kV, ± 15 kV
dans l’air
Transitoires
électriques
rapides/
salves
CEI 61000-
4-4
± 0,5 kV,
± 1 kV, ± 2 kV
pour les lignes
d’alimentation
électrique
Fréquence de
répétition de
100 kHz
± 0,5 kV,
± 1 kV, ± 2 kV
pour les lignes
d’alimentation
électrique
Fréquence de
répétition de
100 kHz
La qualité de l’alimenta-
tion secteur doit
correspondre à celle
d’un environnement
commercial ou d’un
milieu hospitalier type.
Surtension
CEI 61000-
4-5
± 0,5 kV,
± 1 kV ligne(s)
à ligne(s)
± 0,5 kV,
± 1 kV ligne(s)
à ligne(s)
La qualité de l’alimenta-
tion secteur doit
correspondre à celle
d’un environnement
commercial ou d’un
milieu hospitalier type.
± 0,5 kV,
± 1 kV,
± 2 kV ligne(s)
à terre
± 0,5 kV,
± 1 kV,
± 2 kV ligne(s)
à terre
Creux de
tension,
coupures
brèves et
variations
de tension
sur les
lignes d’ali-
mentation
électrique
CEI 61000-
4-11
0 % d’UT ;
0,5 cycle à 0°,
45°, 90°, 135°,
180°, 225°,
270° et 315°
0 % d’UT ;
0,5 cycle à 0°,
45°, 90°, 135°,
180°, 225°,
270° et 315°
La qualité de
l’alimentation secteur
doit correspondre à
celle d’un environnement
commercial ou d’un
milieu hospitalier
type. Si l’utilisateur du
contrôleur RF NovaSure
doit maintenir la
continuité du
fonctionnement pendant
les coupures de courant,
il est recommandé
d’alimenter le contrôleur
RF NovaSure par le biais
d’un onduleur ou d’une
batterie.
0 % d’UT ;
1 cycle et
70 % d’UT ;
25/30 cycles
Monophase :
à 0°
0 % d’UT ;
1 cycle et
70 % d’UT ;
25/30 cycles
Monophase :
à 0°
0 % d’UT ;
250 cycles
0 % d’UT ;
250 cycles
Cette situation
entraîne l’arrêt
du contrôleur
RF, puis son
retour au
mode Standby
(Veille).
Fréquence
du réseau
50/60 Hz
Champ
magnétique
CEI 61000-
4-8
30 A/m
50 Hz
30 A/m
50 Hz
Les niveaux des
champs magnétiques à
la fréquence du réseau
doivent correspondre à
ceux d’un environnement
commercial ou d’un
milieu hospitalier type.
Remarque : UT représente la tension en c.a. du secteur avant l’application du niveau
d’essai.

24
FRANÇAIS
REMARQUE1: à 80 MHz et 800 MHz, c’est la plage des fréquences
supérieures qui s’applique.
REMARQUE2: ces recommandations peuvent ne pas s’appliquer à
toutes les situations. La propagation électromagnétique est affectée par
l’absorption et le réfléchissement des structures, objets et individus.
a
Les intensités de champ en provenance d’émetteurs fixes, tels que les stations de base pour
radiotéléphones (portables/sans fil) et les radios mobiles terrestres, radios-amateurs, émissions de radio AM
et FM et émissions de télévision, ne peuvent théoriquement pas être prévues de façon précise. Pour évaluer
l’environnement électromagnétique dû aux émetteurs RF fixes, une étude électromagnétique sur site doit
être envisagée. Si l’intensité de champ mesurée à l’endroit où le générateur RF est utilisé dépasse le niveau
de conformité RF applicable ci-dessus, le générateur RF doit être observé afin de vérifier qu’il fonctionne
normalement. Si l’on constate des prestations anormales, d’autres mesures peuvent être nécessaires,
comme la réorientation ou le déplacement du générateur RF.
b
Au-delà de la plage de fréquences de 150 kHz à 80 MHz, les intensités de champ doivent être inférieures
à 3 V/m.
Distances de séparation recommandées entre les équipements
de communication RF portables et mobiles etle contrôleur RF
NovaSure
L’équipement de communication RF portable (y compris les
périphériques tels que les câbles d’antenne et les antennes externes)
ne doit pas être utilisé à moins de 30cm de toute partie du système
d’ablation de l’endomètre à impédance contrôlée NovaSure, y compris
les câbles spécifiés par Hologic Inc. Sinon, une dégradation de la
performance de cet équipement pourrait en résulter.
Nettoyage et désinfection
Il est recommandé d’employer des agents non inflammables pour le
nettoyage et la désinfection. Les agents inflammables ou les solvants
utilisés pour le nettoyage ou la désinfection doivent pouvoir s’évaporer
avant d’utiliser le système NovaSure.
Le contrôleur RF NovaSure n’est pas stérile. Le nettoyage doit s’effectuer
au moyen d’un détergent doux et d’une solution aqueuse pour essuyer
uniquement les surfaces. Ne pas plonger l’appareil dans du liquide, ni
introduire de liquide dans les aérations ou les zones de câbles RF.
Le dispositif jetable NovaSure est stérile et exclusivement à usage unique.
• Ne pas utiliser si son emballage a été ouvert ou endommagé.
• Ne pas réutiliser ou restériliser le dispositif jetable.
Ne stériliser aucun composant du système d’ablation de l’endomètre
contrôlée par impédance NovaSure.
Tableau 3 - Recommandations et déclaration du fabricant –
Immunité électromagnétique
Recommandations et déclaration du fabricant – Immunité
électromagnétique
Le contrôleur RF NovaSure est conçu pour fonctionner dans l’environnement
électromagnétique précisé ci-dessous. Le client ou l’utilisateur du contrôleur RF
NovaSure doit s’assurer qu’il est utilisé dans cet environnement.
Test
d’immunité CEI 60601
Niveau d’essai Conformité
Niveau
Environnement électro-
magnétique – Recomman-
dations
RF conduites
CEI 61000-
4-6
3 V
0,15 MHz à
80 MHz
6 V dans les
bandes ISM et
les bandes radios
amateurs entre
0,15 MHz et
80 MHz
80 % d’AM à
1 kHz
3 V
0,15 MHz à
80 MHz
6 V dans les
bandes ISM
et les bandes
radios amateurs
entre
0,15 MHz et
80 MHz
80 % d’AM à
1 kHz
RF rayonnées
CEI 61000-
4-3
3 V/m
80 MHz à
2,7 GHz
80 % d’AM à
1 kHz
3 V/m
80 MHz à
2,7 GHz
80 % d’AM à
1 kHz
Distance de séparation
minimale recommandée
L’équipement de
communication RF portable
(y compris les périphériques
tels que les câbles
d’antenne et les antennes
externes) ne doit pas être
utilisé à moins de 30cm
de toute partie du système
d’ablation de l’endomètre
à impédance contrôlée
NovaSure, y compris les
câbles spécifiés par Hologic
Inc. Sinon, une dégradation
de la performance de cet
équipement pourrait en
résulter.
Les intensités de
champ en provenance
d’émetteurs RF fixes, telles
que déterminées par une
étude
électromagnétique sur site
a
,
doivent être inférieures au
niveau de conformité dans
chaque plage de fréquences.
b
Des interférences peuvent se
produire à proximité d’appareils
marqués du symbole suivant :

25
FRANÇAIS
Liste des pièces
Informations de commande et pièces et accessoires correspondants
Référence du produit Description
RFC2010 Contrôleur RF NovaSure, Modèle 10
814002 Cordon d’alimentation, 115 volts, Amérique du Nord
814003 Cordon d’alimentation, 230 volts, Europe
814004 Cordon d’alimentation, 220 volts, Royaume-Uni/
Irlande
814005 Cordon d’alimentation, Danemark
814009 Cordon d’alimentation, Italie
814011 Cordon d’alimentation, Suisse
814015 Cordon d’alimentation, Japon
814016 Cordon d’alimentation, Australie
52124-001 Pédale
815012 CO2 (Pharmacopée américaine ou USP), paquet de
5cartouches
NS2013 Kit de dispositif jetable d’ablation de l’endomètre
300001 contrôlée par impédance NovaSure
Élimination
Mise en garde: Le dispositif jetable usagé doit être traité
comme un déchet représentant un risque biologique et mis au
rebut conformément aux pratiques standard de l’hôpital ou de
la clinique où le traitement est effectué.
Hologic et ses distributeurs et clients dans la Communauté européenne
sont tenus de respecter la directive relative aux déchets d’équipements
électriques et électroniques (DEEE) (2002/96/CE). Hologic s’engage à
respecter les exigences nationales concernant le traitement respectueux
de l’environnement de ses produits. L’objectif d’Hologic est de réduire
les déchets résultant de l’élimination des équipements électriques et
électroniques. Hologic est conscient des bénéfices que l’on peut tirer
de la réutilisation, du traitement, du recyclage ou de la récupération
éventuels de ces DEEE afin de minimiser la quantité de substances
dangereuses libérées dans l’environnement. Les clients d’Hologic dans
la Communauté européenne doivent veiller à ce que les dispositifs
portant le symbole suivant, qui indique que la directive DEEE s’applique,
ne soient pas placés dans un système municipal de traitement des
déchets, sauf lorsque les autorités locales l’autorisent.
Contacter l’assistance technique d’Hologic pour organiser l’élimination
correcte du contrôleur RF conformément à la directive DEEE.
Garantie
Sauf mention expresse contraire dans l’Accord : i) Hologic garantit
au Client initial que l’équipement qu’elle fabrique fonctionnera
conformément aux spécifications produit publiées et ce, pendant un
(1) an à compter de la date d’expédition ou, si une installation est
nécessaire, à partir de la date d’installation (« Période de garantie »)
; ii) les tubes à rayons X utilisés pour la mammographie numérique
sont garantis pendant vingt-quatre (24) mois, à savoir garantis à 100
% pendant les douze (12) premiers mois et garantis au prorata de la
vétusté pendant les mois 13 à 24 ; iii) les pièces de rechange et les
éléments reconditionnés sont garantis pendant le reste de la Période de
garantie ou quatre-vingt-dix (90) jours à compter de l’expédition, selon
le délai le plus long ; iv) les consommables sont garantis conformes aux
spécifications publiées pendant une période prenant fin à la date de
péremption indiquée sur leur emballage respectif ; v) le Logiciel sous
licence est garanti pour un fonctionnement conforme aux spécifications
publiées ; vi) Hologic garantit que les services sont exécutés dans les
règles de l’art ; vii) l’équipement non fabriqué par Hologic est garanti par
le fabricant concerné et ladite garantie peut s’étendre aux clients Hologic
dans les limites autorisées par le fabricant de cet équipement non
fabriqué par Hologic. Hologic ne garantit pas que les produits pourront
être utilisés en continu ou sans erreur, ni que les produits fonctionneront
avec des produits tiers non agréés par Hologic.
Ces garanties ne s’appliquent pas à un élément ayant été :
(a) réparé, déplacé ou modifié par des personnes autres que le personnel
de maintenance agréé par Hologic ; (b) soumis à des contraintes
physiques (y compris thermiques ou électriques), des conditions
d’utilisation extrêmes ou un usage inapproprié ;
(c) conservé, entretenu ou utilisé ne respectant pas les spécifications
ou instructions Hologic applicables, ce qui inclut le refus d’installer les
mises à niveau logicielles recommandées par Hologic ; ou (d) désigné
comme un produit fourni sous une garantie autre que celle accordée par
Hologic, un prototype ou un produit d’occasion.
Assistance technique et informations pour le renvoi du
produit
Avertissement: la chute du contrôleur RF annule la garantie et
risque de l’endommager au point où il ne pourrait pas être réparé.
Nous recommandons vivement l’utilisation d’un chariot stable sur
lequel le contrôleur sera maintenu ou fixé afin de réduire les risques
de chute. Se montrer tout particulièrement prudent lors du transport
du contrôleur RF hors du site.
Pour toute question au sujet du contrôleur RF, contacter le
+1-800-442-9892 ou le +1-508-263-2900.
Représentants du service après-vente
Si le contrôleur RF NovaSure cesse de fonctionner, contacter l’assistance
technique d’Hologic pour recevoir des instructions et un numéro
d’autorisation de renvoi de matériel (N° RMA). Nettoyer et réemballer
correctement le contrôleur, puis le renvoyer pour réparation ou dépannage
à l’une des adresses agréées indiquées ci-dessous. Si le contrôleur RF
NovaSure n’est plus sous garantie, le montant correspondant aux frais
divers et à la réparation sera établi dès réception et inspection de l’appareil.

26
FRANÇAIS
Glossaire de symboles
Symbole
Référence
standard et
numéro de
symbole
Titre du sym-
bole Description du symbole
EN ISO 15223-
1, 5.1.2
Mandataire
agréé dans la
Communauté
européenne
Indique le représentant
autorisé dans la Commu-
nauté européenne.
CEI 60601-1,
Tableau D.1, 1
IEC 60417,
5032
Courant alterna-
tif (CA)
Indique sur la plaque
signalétique que
l’équipement est adapté
au courant alternatif
seulement; pour identifier
les terminaux pertinents.
EN ISO 15223-
1, 5.3.9
ISO 7000, 2621
Limites de pres-
sion atmosphéri-
que
Indique la plage de
pression atmosphérique
à laquelle le dispositif
médical peut être exposé
en toute sécurité.
EN ISO 15223-
1, 5.1.5
ISO 7000, 2492
Code du lot Indique le code de lot du
fabricant afin que le lot
puisse être identifié.
CO2NA Dioxyde de
carbone Indique le dioxyde de
carbone.
EN ISO 15223-
1, 5.1.6
ISO 7000, 2493
Référence du
catalogue
Indique la référence cata-
logue du fabricant afin
que le dispositif médical
puisse être identifié.
N/A Appareil de caté-
gorie non-PA Pour identifier la catégorie
d’équipement non AP.
EN ISO 15223-
1, 5.4.4
ISO 7000,
0434A
CEI 60601-1,
Tableau D.1, 10
Mise en garde
Pour indiquer qu’il faut
être prudent lors de l’uti-
lisation du dispositif ou
du contrôle à proximité de
l’endroit où le symbole est
placé, ou pour indiquer
que la situation actuelle
nécessite l’attention ou
une action de l’opérateur
afin d’éviter des consé-
quences indésirables.
Directive
médicale euro-
péenne 93/42/
CEE, article 17
et annexe XII
Règlement
européen
2017/745 sur
les dispositifs
médicaux,
annexe V
Marque de
conformité CE
avec numéro
d’identification
de l’organisme
notifié
Indique que le dispositif
médical est conforme
à la directive médicale
européenne 93/42/CEE
et répond aux exigences
applicables en matière de
santé, de sécurité et d’en-
vironnement. Si la marque
est accompagnée d’un
numéro, la conformité est
vérifiée par l’organisme
notifié indiqué.
Informations complémentaires
Pour toute demande d’assistance ou pour obtenir des informations de
commande aux États-Unis, veuillez contacter :
Hologic, Inc.
250 Campus Drive
Marlborough, MA 01752 ÉTATS-UNIS
Téléphone : +1-800-442-9892 (numéro d’appel gratuit)
www.hologic.com
Remarque: tout incident ou problème qui pourrait représenter un
risque pour la sécurité doit être signalé à l’assistance technique
d’Hologic.
Hologic BV
Da Vincilaan 5
1930 Zaventem
Belgium
Tel: +32 2 711 46 80
Fax: +32 2 725 20 87
Signalez à Hologic toute réclamation ou tout problème relatifs à la
qualité, la fiabilité, la sécurité ou aux performances du produit. Si
le dispositif a causé ou aggravé une blessure du patient, signalez
immédiatement l’incident au représentant autorisé Hologic et
à l’autorité compétente de l’État membre ou du pays concerné.
Les autorités compétentes, pour les dispositifs médicaux, sont
généralement le ministère de la Santé de chaque État membre ou
une agence au sein du ministère de la Santé.
Renvois au service après-vente
Lire les instructions ci-dessous avant de renvoyer tout produit
potentiellement défectueux utilisé/non utilisé à Hologic.
Contacter l’assistance technique d’Hologic si le dispositif jetable
NovaSure ou le contrôleur RF NovaSure ne fonctionne pas comme
prévu. Lors du renvoi d’un produit à Hologic, quelle qu’en soit la raison,
l’assistance technique émettra un numéro d’autorisation de renvoi de
matériel (RMA) et un kit de danger biologique, le cas échéant.
Renvoyer les contrôleurs RF en respectant les instructions fournies
par l’assistance technique. Bien nettoyer le contrôleur RF avant de
le renvoyer et renvoyer tous les accessoires dans l’emballage avec
l’unitérenvoyée.
Renvoyer les dispositifs jetables utilisés ou ouverts en suivant les
instructions fournies avec le kit de danger biologique fourni par Hologic.

27
FRANÇAIS
Symbole
Référence
standard et
numéro de
symbole
Titre du sym-
bole Description du symbole
EN ISO 15223-
1, 5.4.3
ISO 7000, 1641
CEI 60601-1,
Tableau D.1, 11
Consulter le
mode d’emploi
Indique la nécessité pour
l’utilisateur de consulter le
mode d’emploi.
CC
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 6049
Pays de fabrica-
tion Identifie le pays de fabri-
cation des produits.
CEI 60601-1,
Tableau D.1, 24
CEI 60417,
5036
Tension dan-
gereuse
Indique les dangers
découlant de tensions
dangereuses
EN ISO 15223-
1, 5.1.3
ISO 7000, 2497
Date de fabrica-
tion
Indique la date à laquelle
le dispositif médical a été
fabriqué.
CEI 60601-1,
Tableau D.1, 26
CEI 60417,
5334
Appareil de type
BF résistant aux
défibrillations
Identifie une pièce ap-
pliquée de type BF résis-
tante à la défibrillation
conforme à la norme CEI
60601-1.
EN ISO 15223-
1, 5.2.6
ISO 7000, 2608
Ne pas restéri-
liser
Indique un dispositif
médical qui ne doit pas
être restérilisé.
EN ISO 15223-
1, 5.4.2
ISO 7000, 1051
CEI 60601-1,
Tableau D.1, 28
Ne pas réutiliser Indique un dispositif
médical qui est destiné à
un usage unique.
ISO 7000, 2403
ISO 780
Ne pas empiler
au-dessus d’une
hauteur « n »
Indique que les éléments
ne doivent pas être
empilés verticalement
au-delà du nombre spéci-
fié, soit en raison de la
nature de l’emballage de
transport, soit en raison
de la nature des éléments
eux-mêmes.
EN ISO 15223-
1, 5.2.8
ISO 7000, 2606
Ne pas utiliser si
l’emballage est
endommag
Indique un dispositif
médical qui ne doit pas
être utilisé si l’emballage
a été endommagé ou
ouvert et que l’utilisateur
doit consulter le mode
d’emploi pour obtenir des
informations supplémen-
taires.
Symbole
Référence
standard et
numéro de
symbole
Titre du sym-
bole Description du symbole
IEC 60601-1,
Tableau D.1, 8
CEI 60417,
5021
Borne d’équi-
potentialité
Identifie les bornes qui,
lorsqu’elles sont connec-
tées ensemble, amènent
les différentes parties
d’un équipement ou d’un
système au même poten-
tiel, sans nécessairement
être le potentiel de terre
(masse), par exemple pour
la connexion locale.
Directive DEEE
2002/96/EC
2012/19/EC
EN 60417,
6414
Directive de la
Communauté
européenne rela-
tive aux déchets
d’équipements
électriques et
électroniques
(DEEE) 2002/96/
CE
Indique que la collecte
séparée des déchets
d’équipements électriques
et électroniques (DEEE)
est nécessaire.
IEC 60417,
5114 Pédale Identifie un interrupteur
au pied ou la connexion
d’un interrupteur au pied.
ISO 7010
ISO 3864-2,
M002
Suivre le mode
d’emploi
Signifie que le manuel/
la brochure d’instructions
doit être lu(e).
EN ISO 15223-
1, 5.3.1
ISO 7000, 0621
ISO 780
Fragile
Indique un dispositif
médical qui peut être
cassé ou endommagé s’il
n’est pas manipulé avec
soin.
CEI 60143-1,
5016 Fusible Identifie les boîtes à
fusibles ou leur emplace-
ment.
HP N/A Haute pression Indique une pression
élevée.
EN ISO 15223-
1, 5.3.8
ISO 7000, 2620
Limites
d’humidité
Indique la plage d’humi-
dité à laquelle le dispositif
médical peut être exposé
en toute sécurité.
EN ISO 15223-
1, 5.3.2
ISO 7000, 0624
ISO 780
Protéger de la
chaleur
Indique un dispositif
médical qui doit être
protégé des sources de
chaleur.
EN ISO 15223-
1, 5.3.4
ISO 7000, 0626
ISO 780
Conserver au sec Indique un dispositif mé-
dical qui doit être protégé
de l’humidité.

28
FRANÇAIS
Symbole
Référence
standard et
numéro de
symbole
Titre du sym-
bole Description du symbole
EN ISO 15223-
1, 5.1.1
ISO 7000, 3082
Fabricant Indique le fabricant du
dispositif médical.
ISO/DIS 15223-
1, 5.7.7 Dispositif médica Indique que l’élément est
un dispositif médical.
N/A Sans huile Indique qu’il n’y a pas
d’huile.
EN ISO 15223-
1, 5.2.7
ISO 7000, 2609
Non stérile
Indique un dispositif
médical qui n’a pas été
soumis à un processus de
stérilisation.
LATEX EN ISO 15223-
1, Annexe B
Fabriqué sans
latex de caou-
tchouc naturel
Indique l’absence de
caoutchouc naturel sec
ou de latex de caoutchouc
naturel.
ISO 7000, 2794 Unité
d’emballage Indique le nombre
d’unités dans un paquet.
FDA 21 CFR
801
Utilisation sur
ordonnance
seulement
Mise en garde: La loi
fèdèrale (des États-unis)
limite la vente de ce
dispositif par un mèdecin
formè á son utilistion ou
sure ordonnance.
IEC 60417,
5140
Rayonnement
électro-ma-
gnétique non
ionisant
Pour indiquer des niveaux
généralement élevés,
potentielle-ment dange-
reux, de rayonnement non
ionisant, ou pour indiquer
des équipements ou des
systèmes, par exemple
dans le domaine de
l’électricité médicale, qui
comprennent des émet-
teurs RF ou qui appliquent
intentionnelle-ment de
l’énergie électro-magné-
tique RF pour le diagnos-
tic ou le traitement.
EN ISO 15223-
1, 5.1.7
ISO 7000, 2498
Numéro de série
Indique le numéro de
série du fabricant afin de
permettre l’identification
d’un dispositif médical
spécifique
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 3707
Système de
barrière stérile
unique
Indique un système de
barrière stérile unique.
Symbole
Référence
standard et
numéro de
symbole
Titre du sym-
bole Description du symbole
EN ISO 15223-
1, 5.2.3
ISO 7000, 2501
NuméroStéri-
lisé à l’oxyde
d’éthylène de
série
Indique un dispositif
médical qui a été stérilisé
à l’oxyde d’éthylène.
EN ISO 15223-
1, 5.3.7
ISO 7000, 0632
Limites de tém-
pérature
Indique les limites de
température auxquelles
le dispositif médical peut
être exposé en toute
sécurité.
ISO 7000, 0623
ISO 780, 0623
IATA 2004
Ce côté en haut Indique la position verti-
cale correcte de l’embal-
lage de transport.
ISO/DIS 15223-
1, 5.7.10 Identifiant
d’appareil unique
Indique les identifiants
d’appareil et les identifi-
ants de production du
dispositif médical.
EN ISO 15223-
1, 5.1.4
ISO 7000, 2607
Date de péremp-
tion
Indique la date après la-
quelle le dispositif médical
ne doit plus être utilisé.
Hologic, NovaSure et les logos associés sont des marques de commerce
et/ou des marques déposées d’Hologic, Inc. et/ou de ses filiales aux
États-Unis et/ou dans d’autres pays.
Le système d’ablation de l’endomètre contrôlée par impédance NovaSure
est fabriqué et distribué par Hologic, Inc.
© 2014-2022 Hologic, Inc.
AW-22724-901 Rev. 001
04/2022

1
DEUTSCH
NovaSure®
Gebrauchsanweisung und
Betriebshandbuch für den Controller
Inhalt
Checkliste für Ärzte ..................................1
Beschreibung des Systems ............................1
Indikationen ........................................3
Patientenzielgruppe ..................................3
Vorgesehener klinischer Nutzen für Patienten ..............3
Vorgesehene Benutzer ................................3
Kontraindikationen ...................................3
Warnhinweise ....................................... 4
Vorsichtsmassnahmen ................................5
NovaSure-Daten einer dreijährigen Studie ................6
Nebenwirkungen ..................................6
Nach dem Verfahren zu erwartende Komplikationen ....... 7
Weitere Nebenwirkungen ............................ 7
Klinische Studie ...................................7
Patientenauswahl .................................9
Patientenberatung ................................10
Vorbereitung der Patientin auf die Behandlung ............10
NovaSure Impedanzgesteuertes Endometrium ............10
Betrieb des HF-Controllers, Modell 10 ................16
Regelmäßige Wartung und Reparatur .................17
Bildschirmsymbole des NovaSure HF-Controllers, Modell 10 18
Zusätzliche Fehlerbehebungsmaßnahmen .............18
Anweisungen zum Auswechseln von Ersatzteilen ..........20
Technische Spezifikationen ...........................21
NovaSure-Einmalinstrument ........................21
NovaSure HF-Controller ............................ 21
Umgebungsbedingungen ...........................22
Wichtige Leistungsmerkmale .......................22
Elektromagnetische Sicherheit – Leitlinien .............22
Reinigung und Desinfektion .........................24
Teileliste ........................................25
Entsorgung ........................................25
Garantie ..........................................25
Technischer Kundendienst und Informationen .............25
Glossar der Symbole ................................26
VORSICHT: LAUT US-BUNDESBEHÖRDE DARF DIESES PRODUKT
NUR VON EINEM ARZT ODER IM AUFTRAG EINES ARZTES MIT
ENTSPRECHENDER SCHULUNG ERWORBEN WERDEN.
Vor der Verwendung alle Anweisungen, Vorsichtsmaßnahmen
und Warnhinweise lesen. Eine Nichtbefolgung der Anweisungen,
Warnhinweise oder Vorsichtsmaßnahmen könnte zu einer
ernsthaften Verletzung der Patientin führen.
Hinweis: Das dem Einmalinstrument beiliegende Handbuch enthält
möglicherweise eine aktuellere Überarbeitung der Anweisungen zum
NovaSure-System als das dem Controller beiliegende Handbuch.
Das NovaSure-Einmalinstrument ist nicht zur Verwendung mit
anderen Controllern und/oder HF-Generatoren bestimmt, und der
NovaSure-HF-Controller ist nicht zur Verwendung mit anderen
Einmalinstrumenten bestimmt.
Das NovaSure-Einmalinstrument enthält kein Latex.
Checkliste für Ärzte
Der Arzt muss:
• über ausreichende Erfahrung in der Durchführung von Verfahren
innerhalb der Uterushöhle, wie beispielsweise Einsetzen eines
Intrauterinpessars (IUD) oder Dilatation und Kürettage (D&C)
sowie über eine angemessene Schulung und Kenntnisse über die
Verwendung des NovaSure-Systems verfügen und mit dem System
vertraut sein.
• die Anweisungen einsehen und sich damit vertraut machen und
entweder an einer NovaSure-Schulung teilnehmen oder von einem
qualifizierten Arzt unterwiesen werden.
• sich der angemessenen Abfolge von Schritten bewusst sein, auf die
in der Bedienungsanleitung und im Abschnitt zur Fehlerbehebung in
diesem Handbuch eingegangen wird. Sie betreffen das Abbrechen,
Korrigieren bzw. Fortsetzen der Behandlung bei Ermittlung von
CO2-Verlust während des Perforationstests zur Überprüfung der
Integrität des Uterus und einer möglichen Uterusperforation.
Hilfspersonal muss sich vor Einsatz des NovaSure-Systems mit diesen
Anweisungen und anderem Schulungsmaterial vertraut machen.
Beschreibung des Systems
Das NovaSure Impedanzgesteuerte Endometrium-Ablationssystem
besteht aus dem NovaSure-Einmalinstrument mit Verbindungskabel,
NovaSure HF-Controller, NovaSure-CO2-Kanister, Trockenmittelfilter,
Fußschalter und Netzkabel, die zur gemeinsamen Verwendung als
System bestimmt sind.

2
DEUTSCH
NovaSure-Einmalinstrument mit Verbindungskabel,
inkl.Trockenmittelfilter für Absaugleitung
Beschreibung des NovaSure-Einmalinstruments
Das NovaSure-Einmalinstrument besteht aus einer anpassbaren,
bipolaren Goldnetzelektrode, die zur Verwendung bei nur einer Patientin
bestimmt ist, auf einem ausfahrbaren Rahmen befestigt ist und eine
Läsion über dem gesamten inneren Oberflächenbereich der Uterushöhle
verursachen kann. Das Einmalinstrument wird durch den Uterushals in
die Uterushöhle eingeführt. Die Hülse wird dann zurückgezogen, so dass
sich die bipolare Goldnetzelektrode entfalten und an die Uterushöhle
anpassen kann.
Die bipolare Goldnetzelektrode besteht aus einem metallbeschichteten,
porösen Stoff, durch den kontinuierlich Dampf und Feuchtigkeit aus dem
ausgetrockneten Gewebe abgesaugt werden. Das Einmalinstrument
führt in Verbindung mit einem dedizierten NovaSure HF-Controller in
durchschnittlich ca. 90Sekunden eine individuell angepasste, globale
Endometriumablation durch, ohne eine gleichzeitige hysteroskopische
Visualisierung oder eine Vorbehandlung des Endometriums erforderlich
zu machen. Die spezielle Konfiguration der bipolaren Goldnetzelektrode
und die voreingestellte Leistung des Controllers bewirken eine
kontrollierte Ablationstiefe im Uterus, deren Ultraschallmessung bis zu
10cm und deren Cornu-zu-Cornu-Abstand mindestens 2,5cm beträgt.
Während des Ablationsvorgangs wird das Endometrium ungeachtet
seiner Dicke durch die abgegebene Hochfrequenzenergie (HF) vaporisiert
bzw. verödet. Das darunter liegende, oberflächliche Myometrium wird
ausgetrocknet und verödet.
Der Controller berechnet gemäß der Uterusgröße automatisch die
optimale Leistungsstufe (W), die zur Behandlung der Uterushöhle
erforderlich ist. Wenn die Gewebezerstörung eine optimale Tiefe erreicht,
wird der Controller durch den verstärkten Gewebewiderstand dazu
veranlasst, die Energieabgabe automatisch abzubrechen, wodurch ein
selbstregulierender Vorgang gegeben ist. Blut, Kochsalzlösung und
andere, zum Zeitpunkt des Verfahrens in der Uterushöhle vorhandene
Flüssigkeiten sowie die vom ausgetrockneten Gewebe freigesetzten
Dämpfe werden durch kontinuierliches, automatisches Absaugen
entfernt. Das Einmalinstrument ist mit dem Controller über ein Kabel
verbunden.
In diesem Kabel befinden sich das HF-Kabel, der Absaugschlauch, der
während des Zyklus zur Beurteilung der Intaktheit der Uterushöhle
zur Drucküberwachung und während des Ablationszyklus zum
Absaugen bestimmt ist, und der Vakuum-Rückführungsschlauch, der
während des Zyklus zur Beurteilung derIntaktheit der Uterushöhle
zur Kohlendioxidzufuhr und während des Ablationszyklus zur
Vakuumüberwachung bestimmt ist. Das Einweggerät wurde mit
Ethylenoxid (EO) sterilisiert.
NovaSure HF-Controller,
Modell 10
Beschreibung des NovaSure HF-Controllers
Der NovaSure HF-Controller erzeugt kontinuierlich abgegebene Energie
und ist zur Abgabe einer maximalen Nennleistung von 180 Watt fähig.
Der Controller berechnet die Energieabgabe automatisch gemäß der
Längenmessung der Uterushöhle (Ultraschallmessung minus Länge
des Uterushalskanals) und der Breitenmessung, die vom Benutzer über
die Tasten am Controller eingegeben wird. Durch Überwachung des
Gewebewiderstands während des Ablationsvorgangs wird die Tiefe
der Endometrium- und Myometrium-Ablation automatisch gesteuert.
Das NovaSure-Verfahren schaltete automatisch ab, sobald bei der
Endometriumverdampfung und der oberflächlichen myometrialen
Austrocknung an der Schnittstelle zwischen Gewebe und Elektrode
eine Impedanz von etwa 50Ohm erreicht wurde oder wenn die
Anwendungszeit von zwei Minuten abgelaufen ist. Im Controller
ist ein Perforationstest integriert, ein System, das zur Feststellung
eines Defekts oder einer Uteruswandperforation konzipiert wurde.
Nachdem das Einmalinstrument in die Uterushöhle eingeführt
wurde, wird der Uterushöhle mit sicherer Flussrate und sicherem
Druck über den Vakuum-Rückführungsschlauch im mittleren Lumen
des Einmalinstruments CO2 zugeführt. Wenn der CO2-Druck in der
Uterushöhle für kurze Zeit aufrechterhalten wird, woran zu erkennen ist,
dass die Uterushöhle intakt ist, gestattet das System zur Beurteilung der
Intaktheit der Uterushöhle die Aktivierung des NovaSure HF-Controllers
und den Beginn der Behandlungsphase. Während des gesamten
Endometrium-Ablationsverfahrens wird mit einer Vakuumpumpe
im NovaSure HF-Controller ein Vakuum in der Uterushöhle erzeugt
und aufrechterhalten. Die Vakuumstufe wird während des gesamten
Ablationsvorgangs überwacht.

3
DEUTSCH
Beschreibung des Trockenmittelfilters
der NovaSure-Absaugleitung
Der Trockenmittelfilter für die NovaSure-
Absaugleitung ist eine unsterile, zur
Verwendung bei nur einer Patientin
bestimmte Komponente, die der Benutzer
am Absaugschlauch befestigt, bevor
das Einmalinstrument an den NovaSure
HF-Controller angeschlossen wird. Das
Trockenmittel absorbiert die Feuchtigkeit,
die während des Ablationsverfahrens
über den Absaugschlauch aus der
Uterushöhle entfernt wird.
Beschreibung des NovaSure-
Fußschalters
Der NovaSure-Fußschalter ist ein
pneumatischer Schalter, der an
derVorderseite des NovaSure
HF-Controllers angeschlossen wird.
Er dient zur Aktivierung des NovaSure
HF-Controllers und enthält keine
elektrischen Komponenten.
Beschreibung des NovaSure
CO2-Kanisters
Der NovaSure CO2-Kanister enthält
16Gramm CO2 medizinischer Güte.
Erwird an den Regler an derRückseite
des NovaSure HF-Controllers
angeschlossen, bevor Netzspannung an
den NovaSure HF-Controller angelegt
wird. Der Perforationsdetektor setzt die
Uterushöhle mit CO2 unter Druck.
Der CO2 -Kanister Art.-Nr.: 815012 ist
99% CO2.
Beschreibung des NovaSure-
Wechselstromkabels
Das NovaSure-Wechselstromkabel ist
ein Netzkabel medizinischer Güte und
versorgt den NovaSure HF-Controller mit
geeigneter Netzspannung. Die Buchse für
das Netzkabel, das Stromeingangsmodul,
befindet sich an der Rückseite des
NovaSure HF-Controllers.
Indikationen
Das NovaSure-System ist zur Ablation der Endometrium-Zellschicht des
Uterus bei Frauen in der Prä-Menopause mit Menorrhagie (sehr starker
Monatsblutung) aufgrund gutartiger Ursachen bestimmt, die keinen
weiteren Kinderwunsch mehr hegen.
Patientenzielgruppe
Das NovaSure-System ist für den Einsatz bei Frauen vor der Menopause
mit Menorrhagie (übermäßiger Blutung) aufgrund gutartiger Ursachen
vorgesehen, die keine Kinder mehr gebären wollen.
Vorgesehener klinischer Nutzen für Patienten
Zur Verringerung oder Beseitigung von Blutungen bei Frauen vor der
Menopause mit schweren Menstruationsblutungen aufgrund gutartiger
Ursachen, die keine Kinder mehr gebären wollen.
Vorgesehene Benutzer
Das NovaSure-System wird unter Aufsicht und Anleitung eines
Gynäkologen oder Chirurgen verwendet. Der Arzt wird in erster Linie das
NovaSure-Gerät bedienen und den Assistenten für die Bedienung der
HF-Steuereinheit und Aktivierung der Steuereinheit mit dem Fußschalter
anweisen. Die HF-Steuereinheit wird nicht steril von einem Assistenten
bedient.
Der Arzt muss:
• ausreichende Erfahrung in der Durchführung von Eingriffen
innerhalb der Gebärmutterhöhle, wie dem Einsetzen einer
Spirale oder Dilatation und Kürettage (Abrasion), haben und über
eine angemessene Ausbildung, ausreichende Kenntnisse und
Vertrautheit mit dem NovaSure-System verfügen.
• mit den Anweisungen zum System vertraut sein oder diese
wiederholen und entweder eine Schulung mit dem NovaSure-
System absolvieren oder von einem qualifizierten Arzt geschult
werden.
Das Hilfspersonal muss mit der Bedienungsanleitung und anderen
Schulungsmaterialien vor der Verwendung des NovaSure-Systems
vertraut sein.
Kontaindikationen
Das NovaSure Impedanzgesteuerte Endometrium-Ablationssystem ist
kontraindiziert zur Verwendung bei:
• Patientinnen, die schwanger sind oder noch schwanger werden
wollen. Schwangerschaften nach einer Ablation können sowohl
für die Mutter als auch für den Fetus gefährlich sein.
• Patientinnen mit einem bekannten oder vermuteten Endometrium-
Karzinom (Uterushalskarzinom) oder Vorstadien bösartiger
Erkrankungen des Endometriums, wie beispielsweise ungelöste
adenomatöse Hyperplasie.
• Patientinnen mit anatomischen Zuständen (wie z. B. ein vertikaler
Kaiserschnitt oder eine transmurale Myomektomie in der Vorgeschichte)
oder pathologischen Zuständen (wie z. B. eine lang anhaltende
medizinische Behandlung), die zu einer Schwächung des Myometriums
führen könnten.
• Patientinnen, die zum Zeitpunkt der Behandlung unter einer aktiven
Genital- oder Harnwegsinfektion leiden (z. B. Zervizitis, Vaginitis,
Endometritis, Salpingitis oder Zystitis).

4
DEUTSCH
• Patientinnen mit einem eingesetzten Intrauterinpessar (IUP).
Das Vorhandensein eines Intrauterinpessars (IUD) in der Uterushöhle
kann das NovaSure-Verfahren beeinträchtigen.
• Patientinnen, deren Uterushöhle weniger als 4 cm lang ist.
DieMindestlänge der Goldnetzelektrode ist 4 cm. Die Behandlung
einer weniger als 4 cm langen Uterushöhle führt zu einer thermischen
Verletzung des Uterushalskanals.
• Patientinnen, deren Uterushöhle weniger als 2,5cm breit ist. Dies lässt
sich anhand der Breitenskala (WIDTH) des Einmalinstruments nach
Einsetzen des Instruments feststellen.
• Patientinnen mit einer akuten Beckenentzündung.
Warnhinweise
Eine Nichtbefolgung der Anweisungen, Warnhinweise oder
Vorsichtsmaßnahmen könnte zu einer ernsthaften Verletzung der
Patientin führen.
Das NovaSure-Einmalinstrument darf nur in Verbindung mit dem
NovaSure HF-Controller eingesetzt werden.
Das NovaSure-Verfahren soll nur einmal während eines
einzelnen operativen Eingriffs durchgeführt werden. Wenn
während desselben operativen Eingriffs mehrere NovaSure-
Behandlungszyklen durchgeführt werden, kann dies zu einer
thermischen Verletzung des Darms führen.
Uterusperforation
• Bei der Sondierung, Dilatation oder Einführung des Einmalinstruments
ist Vorsicht geboten, damit die Uteruswand nicht perforiert wird.
• Wenn sich das Einmalinstrument nicht leicht in den Uterushalskanal
einführen lässt, muss unter Anwendung von klinischem Sachverstand
entschieden werden, ob dieser stärker erweitert werden muss.
• Das NovaSure-System führt einen Perforationstest durch, um die
Intaktheit der Uterushöhle zu bewerten, und gibt bei einer möglichen
Perforation vor der Behandlung als Warnung einen Alarmton ab
(Schritt2.36). (Obwohl dieser Test zur Feststellung von Perforationen
der Uteruswand entwickelt wurde, ist er nur als Indikator zu
verstehen und stellt möglicherweise nicht alle Perforationen
unter allen möglichen Umständen fest. Es muss immer klinischer
Sachverstand angewendet werden.)
• Wenn Verdacht auf eine Uterusperforation besteht, sollte das
Verfahren unverzüglich abgebrochen werden.
• Wenn der Perforationstest nach einer angemessenen Anzahl
von Versuchen der Fehlerbehebung (Schritt 2.36) immer noch
fehlschlägt, muss das Verfahren abgebrochen werden.
• Bei Patientinnen, bei denen der Vorgang aufgrund einer vermuteten
Uteruswandperforation abgebrochen wurde, sollte vor der Entlassung
abgeklärt werden, ob eine Perforation vorliegt.
Allgemeine Hinweise
• Die Endometriumablation mit dem NovaSure-System ist kein
Sterilisationsverfahren. Daher sollte die Patientin über geeignete
Verhütungsmethoden informiert werden.
• Nach einer Endometriumablation besteht weiterhin die Möglichkeit
einer Endometrium-Hyperplasie oder eines Endometrium-
Adenokarzinoms. Sie kann dem Arzt möglicherweise die Erkennung
oder Diagnose eines solchen pathologischen Befundes erschweren.
• Eine Endometriumablation ist nur für Frauen bestimmt, die keinen
Kinderwunsch mehr hegen, da die Wahrscheinlichkeit einer
Schwangerschaft nach dem Verfahren wesentlich geringer ist. Eine
Schwangerschaft nach einer Ablation kann sowohl für die Mutter als
auch für den Fetus gefährlich sein.
• Wird das Endometrium-Ablationsverfahren bei Patientinnen durchgeführt,
die sich zuvor einer Tubenligatur unterzogen haben, besteht bei ihnen ein
größeres Risiko für das Auftreten des Postablationssterilisationssyndroms,
das eine Hysterektomie erforderlich machen kann. Dies kann noch bis zu
10 Jahren nach dem Verfahren auftreten.
• Ein Gesundheitsrisiko kann dann entstehen, wenn das NovaSure-
Verfahren bei Vorhandensein einer thermisch oder elektrisch
leitfähigen Mikrometalleinlage durchgeführt wird, die ungünstig liegt
(z. B. Perforation des Eileiters oder des Myometriums). In diesem Fall
kann Wärme von dem vorgesehenen Behandlungsbereich zu anderem
Gewebe und/oder zu Organen hin abgezogen werden, die mit dem
wärmeleitenden Objekt in Kontakt stehen und die ausreichen kann,
um lokale Verbrennungen zu verursachen. Deshalb muss die korrekte
Lage der Mikrometalleinlage festgestellt werden, bevor das NovaSure-
Verfahren durchgeführt wird.
Technische Hinweise
• Das sterile, zur Verwendung bei nur einer Patientin bestimmte
Einmalinstrument darf nicht verwendet werden, wenn die Verpackung
beschädigt zu sein scheint oder Anzeichen einer Manipulation aufweist.
• Das Einmalinstrument darf nur für eine Patientin benutzt werden. Das
Einmalinstrument darf nicht wiederverwendet oder resterilisiert werden.
Zu den Risiken bei der Wiederverwendung des Einmalinstruments
gehören unter anderem folgende:
• Unwirksamkeit des Verfahrens
• Infektion (größeren Umfangs)
• Stromschlag
• Übertragung ansteckender Krankheiten
• Verletzung des Uterushalses
• Uterusperforation
• Wird direkt vor der NovaSure-Behandlung ein hysteroskopisches
Verfahren mit hypotonischer Kochsalzlösung durchgeführt, muss
die Uterushöhle vor der Behandlung mit dem NovaSure-System mit
physiologischer Kochsalzlösung ausgespült werden. Das Vorhandensein
von hypotonischer Flüssigkeit kann die Wirksamkeit des NovaSure-
Systems beeinträchtigen.

5
DEUTSCH
• Wenn das Einmalinstrument an den Controller angeschlossen wird,
startet der CO2-Fluss zum Entlüften des Einmalinstruments und
der Schläuche. Dieser Entlüftungsvorgang dauert ca. 10Sekunden
und muss mit dem Einmalinstrument außerhalb der Patientin
durchgeführt werden, um der Gefahr einer Luft- oder
Gasembolie vorzubeugen. Auf der HF-Steuereinheit Modell 10
wird eine Spülgerätemeldung angezeigt und während des gesamten
Bereinigungsvorgangs ertönt ein hörbarer pulsierender Ton. Auf
der HF-Steuereinheit Modell 10 wird eine Spülgerätemeldung
angezeigt und während des gesamten Bereinigungsvorgangs ertönt
ein hörbarer pulsierender Ton. Wenn der Ton verstummt und die
LED/Bildschirmmeldung erlischt, kann das Einmalinstrument ohne
Bedenken eingeführt werden.
• Bei Patientinnen mit Herzschrittmachern oder anderen aktiven
Implantaten besteht ein mögliches Risiko, da es zu einer Störung
des Herzschrittmacherbetriebs und zu einer daraus resultierenden
Beschädigung desselben kommen kann. Weitere Informationen vom
Hersteller des Schrittmachers anfordern, wenn die Verwendung des
NovaSure-Systems bei Patientinnen mit einem Herzschrittmacher
vorgesehen ist.
• Es ist darauf zu achten, dass die Patientin keinen Kontakt mit
Metallteilen hat, die geerdet sind oder die eine beträchtliche
Erdungskapazität aufweisen.
• Gefahr: Explosionsgefahr. Nicht in Gegenwart einer entflammbaren
Anästhetikummischung verwenden. Nicht in Gegenwart von
entflammbaren Gasen oder Flüssigkeiten verwenden.
• Ein Versagen des NovaSure-HF-Controllers könnte zu einer
unbeabsichtigten Erhöhung der abgegebenen Energie führen.
Vorsichtsmassnahmen
• In der Fachliteratur wurde berichtet, dass bei Patientinnen mit
einem stark antevertierten, retroflexierten oder lateral verschobenen
Uterus bei intrauterinen Manipulationen ein größeres Risiko einer
Uteruswandperforation besteht.
• Eine falsche Passage kann bei jedem Verfahren entstehen, bei dem
der Uterus mit Instrumenten behandelt wird, insbesondere bei den
Fällen mit einem stark antevertierten, retroflexierten oder lateral
verschobenen Uterus. Es muss vorsichtig vorgegangen werden, um
zu gewährleisten, dass das Instrument richtig in der Uterushöhle
positioniert wird.
• Das NovaSure-System besteht aus den folgenden Komponenten:
- ein zur Verwendung bei nur einer Patientin bestimmtes NovaSure-
Einmalinstrument mit Verbindungskabel
- NovaSure HF-Controller
- NovaSure CO2-Kanister
- NovaSure-Trockenmittelfilter
- NovaSure-Fußschalter
- Netzkabel
Um einen ordnungsgemäßen Betrieb zu gewährleisten, niemals andere
Komponenten mit dem NovaSure-System verwenden. Komponenten
regelmäßig auf Beschädigungen prüfen und Gerät niemals verwenden,
wenn eine Beschädigung erkennbar ist. Die Verwendung von jeglichen
Kabeln oder Zubehörteilen, außer den in diesen Anweisungen
angegebenen, kann zu erhöhten Emissionen oder zu einer verminderten
Sicherheit des HF-Controllers führen.
• Der HF-Controller muss gemäß der Anleitung in diesen
Anweisungen installiert und in Betrieb genommen werden, um seine
elektromagnetische Kompatibilität zu gewährleisten. Siehe die Tabellen
zu den elektromagnetischen Emissionen und zur Störfestigkeit im
Abschnitt Technische Daten.
• Der HF-Controller darf nicht neben oder gestapelt mit anderen Geräten
benutzt werden. Falls eine Verwendung nebeneinander oder gestapelt
erforderlich ist, sollte der HF-Controller beobachtet werden, um den
normalen Betrieb in der Anordnung, in der er verwendet werden wird,
zu überprüfen.
• Tragbare und mobile HF-Kommunikationsgeräte können den HF-
Controller beeinträchtigen. Siehe die Tabellen zur elektromagnetischen
Störfestigkeit im Abschnitt Technische Daten für die empfohlenen
Mindestabstände.
• Patientinnen, die sich einer Endometriumablation unterzogen haben
und später eine Hormonersatztherapie durchführen, sollten in ihre
Medikamentendosis ein Progestin aufnehmen, um dem mit einer
einseitigen Östrogenersatztherapie verbundenen erhöhten Risiko
einesEndometrium-Adenokarzinoms entgegenzuwirken.
• Die Sicherheit und Wirksamkeit des NovaSure-Systems wurde noch
nicht vollständig bewertet bei Patientinnen:
- mit einer Uterus-Ultraschallmessung von mehr als 10 cm;
- mit submukösen Fibromen, die zu einer Entstellung der Uterushöhle
führen;
- mit Uterus bicornis, Uterus septus oder subseptus;
- mit medikamentöser (z. B. GnRH-Agonist) oder chirurgischer
Vorbehandlung;
- die sich früher bereits einer Endometriumablation, einschließlich
des NovaSure-Endometrium-Ablationsverfahrens, unterzogen haben;
oder
- die sich in der Postmenopause befinden.
• Am Controller dürfen bei vermuteten Problemen keine eigenmächtigen
Reparaturen vorgenommen werden. In diesem Fall sollten vom
technischen Kundendienst von Hologic oder einem Verkaufsvertreter
von Hologic telefonisch Anweisungen eingeholt werden.
• Die Kabel zum Einmalinstrument sind so anzuordnen, dass sie nicht
mit der Patientin oder anderen Leitungen in Kontakt kommen.
• Der Benutzer sollte das Einmalinstrument vor der Verwendung auf
Schäden prüfen.
• Der Trockenmittelfilter der Absaugleitung ist unsteril. Die Verpackung
sollte nicht ins sterile Feld gelegt werden.
• Wenn auf dem Bildschirm der HF-Steuereinheit Modell 10 eine ARRAY-
Positionsmeldung angezeigt wird, lesen Sie den Abschnitt Fehlerbehebung
unter „ARRAY-POSITIONSALARM“.

6
DEUTSCH
• Den Trockenmittelfilter für die NovaSure-Absaugleitung nicht
verwenden, wenn es eine rosa Farbe aufweist.
• Das Einmalinstrument muss sich außerhalb der Patientin befinden,
bevor das Kabel in den entsprechenden Anschluss an der Vorderseite
des Controllers (Schritt 2.15) gesteckt wird.
• Das Gas im Kohlendioxidkanister steht unter hohem Druck. Für den
Fall, das ein CO2-Kanister oder eine CO2-Leitung gebrochen ist, den
Kanister vollständig entleeren lassen und den Kanister und/oder
die Leitung auf Raumtemperatur angleichen lassen, bevor damit
gearbeitet wird.
• Vom Anschluss des Einmalinstruments an den Controller bis
zum Abschluss des Uterushöhlen-Beschaffenheitstests strömt
ununterbrochen CO2 aus. Um die Dauer der CO2-Abgabe und eine
mögliche Emboliegefahr so gering wie möglich zu halten, das
Einsetzverfahren sofort nach dem Einführen des Einmalinstruments
durchführen und direkt mit dem Perforationstest fortfahren.
• Leitende Objekte (wie z. B. Überwachungselektroden von anderen
Geräten), die direkten Kontakt mit der Goldnetzelektrode des
Einmalinstruments haben oder sich in unmittelbarer Nähe befinden,
können Strom von der Elektrode ableiten. Dies kann zu lokalen
Verbrennungen der Patientin oder des Arztes oder zu einer Verzerrung
des elektrischen Feldes des Arrays führen, was eine Änderung der
Behandlungswirkung (zu schwache oder zu starke Behandlung) zur
Folge haben würde. Außerdem kann dies zu einer Leistungsverzerrung
in dem anderen leitenden Gegenstand führen, beispielsweise können
Monitore falsche Werte anzeigen.
• Eine zuverlässige Erdung wird nur bei Anschluss des Geräts an eine
für den Krankenhausbetrieb zugelassene Steckdose erzielt.
• Verwenden Sie dieses Gerät nicht in Gegenwart von Magnetquellen
oder in der Nähe von Ultraschall- oder Wärmequellen, um eine
Gefährdung für Anwender und Patienten zu vermeiden.
• Die Zervixmanschette muss vollständig in ihre proximale Position
zurückgezogen sein, um eine mögliche Beschädigung der Hülse beim
Schließen der Elektrode zu minimieren.
• Das NovaSure Instrument ist kontraindiziert für die Verwendung bei
schwangere Frauen oder Frauen, die in Zukunft schwanger werden
möchten. Schwangerschaften nach Ablation können für Mutter und
Fötus gefährlich sein. Eine gründliche medizinische Beurteilung sollte
erfolgen.
NovaSure-Daten einer dreijährigen Studie
Nebenwirkungen
Das NovaSure-System wurde in einer randomisierten, prospektiven,
multizentrischen klinischen Studie ausgewertet, an der 265Patientinnen
mit abnormaler Uterusblutung teilnahmen, wobei das NovaSure-System
zur Kontrolle mit einer Schlingenresektion des Endometriums, gefolgt
von einer Rollerball-Ablation verglichen wurde.
Tabelle 1A. Intraoperative Nebenwirkungen
Nebenwirkung
NovaSure
n=175 (%)
Schlingenresektion
plus Rollerball
n=90 (%)
Bradykardie 1 (0,6 %) 0 (0,0 %)
Uterusperforation 0 (0,0 %) 3 (3,3 %)
Zervixriss 0 (0,0 %) 2 (2,2 %)
Zervixstenose 0 (0,0 %) 1 (1,1 %)
INSGESAMT 1 (0,6 %) 6 (6,7 %)
Tabelle 1B. Postoperative Nebenwirkungen <24 Stunden
Nebenwirkung
NovaSure
n=175 (%)
Schlingenresektion
plus Rollerball
n=90 (%)
Beckenschmerzen/Krämpfe 6 (3,4 %) 4 (4,4 %)
Übelkeit bzw. Erbrechen 3 (1,7 %) 1 (1,1 %)
INSGESAMT 9 (5,1 %)* 5 (5,6 %)**
* Neun gemeldete Fälle bei 6 (3,4 %) Patientinnen
** Fünf gemeldete Fälle bei 4 (4,4 %) Patientinnen
Tabelle 1C. Postoperative Nebenwirkungen >24 Stunden – 2 Wochen
Nebenwirkung
NovaSure
n=175 (%)
Schlingenresektion
plus Rollerball
n=90 (%)
Hämatometra 1 (0,6 %) 0 (0,0 %)
Harnwegsinfektion 1 (0,6 %) 1 (1,1 %)
Scheidenentzündung 1 (0,6 %) 0 (0,0 %)
Endometritis 0 (0,0 %) 2 (2,2 %)
Beckenentzündung 0 (0,0 %) 1 (1,1 %)
Hämorraghie 0 (0,0 %) 1 (1,1 %)
Beckenschmerzen/Krämpfe 1 (0,6 %) 1 (1,1 %)
Übelkeit bzw. Erbrechen 1 (0,6 %) 1 (1,1 %)
INSGESAMT 5 (2,9 %)* 7 (7,8 %)**
* Fünf gemeldete Fälle bei 4 (2,3 %) Patientinnen
** Sieben gemeldete Fälle bei 6 (6,7 %) Patientinnen

7
DEUTSCH
Tabelle 1D. Postoperative Nebenwirkungen >2 Wochen – 1 Jahr
Nebenwirkung
NovaSure
n=175 (%)
Schlingenresektion
plus Rollerball
n=90 (%)
Hysterektomie 3 (1,7 %) 2 (2,2 %)
Hämatometra 1 (0,6 %) 2 (2,2 %)
Harnwegsinfektion 2 (1,1 %) 2 (2,2 %)
Scheidenentzündung 5 (2,9 %) 2 (2,2 %)
Endometritis 2 (1,1 %) 1 (1,1 %)
Beckenentzündung 2 (1,1 %) 0 (0,0 %)
Hämorraghie 1 (0,6 %) 0 (0,0 %)
Beckenschmerzen/Krämpfe 5 (2,9 %) 6 (6,7 %)
INSGESAMT 21 (12,0 %)* 15 (16,17 %)**
* 21 gemeldete Fälle bei 19 (10,9 %) Patientinnen
** 15 gemeldete Fälle bei 15 (16,7 %) Patientinnen
Nach dem Verfahren zu erwartende Komplikationen
Zu den geläufigen postoperativen Nebenwirkungen, die bei
Endometrium-Ablationsverfahren gemeldet werden, gehören:
• Krämpfe/Beckenschmerzen wurden innerhalb von 24 Stunden nach
dem Verfahren bei 3,4 % der NovaSure-Patientinnen und 4,4% der mit
Schlingenresektion plus Rollerball-Ablation behandelten Patientinnen
gemeldet. Postoperativ können leichte bis schwere Krämpfe auftreten.
Diese Krämpfe halten in der Regel einige Stunden lang an und dauern
selten über den ersten Tag nach dem Verfahren fort.
• Übelkeit und Erbrechen wurden innerhalb von 24 Stunden nach dem
Verfahren bei 1,7 % der NovaSure-Patientinnen und 1,1 % der mit
Drahtschlinge plus Rollerball-Ablation behandelten Patientinnen
gemeldet. Wenn überhaupt, treten Übelkeit und Erbrechen in der Regel
direkt im Anschluss an das Verfahren auf, sind auf die Anästhesie
zurückzuführen und können mit Medikamenten behandelt werden.
• Scheidenausfluss
• Scheidenblutung/-schmierblutung
Weitere Nebenwirkungen
Wie bei allen Endometrium-Ablationsverfahren können schwere
Verletzungen oder Tod die Folge sein.
Die folgenden Nebenwirkungen könnten auftreten oder wurden mit der
Verwendung des NovaSure-Systems in Verbindung gebracht:
• Postablationssterilisationssyndrom
• Schwangerschaftsbezogene Komplikationen (Hinweis: Eine
Schwangerschaft nach einer ENDOMETRIUMABLATION istfür
Mutter und Kind sehr gefährlich.)
• Thermische Verletzung des angrenzenden Gewebes
• Uteruswandperforation
• Schwierigkeiten bei der Darm- und Blasenentleerung
• Uterusnekrose
• Luft- oder Gasembolie
• Infektion oder Sepsis
• Komplikationen, die zu schweren Verletzungen oder zum Tod führen
Klinische Studie
Zweck: Es wurden Sicherheit und Wirksamkeit der Verwendung des
NovaSure-Systems mit der Drahtschlingenresektion des Endometriums
gefolgt von einer Rollerball-Ablation bei Frauen in der Prä-Menopause
verglichen, die unter Menorrhagie aufgrund gutartiger Ursachen leiden.
Vorbehandlung: Patientinnen, die nach dem Zufallsprinzip dem NovaSure-
Arm der zweiarmigen Studie zugewiesen wurden, erhielten keine
Vorbehandlung des Endometriums (z. B. Hormone, Dilatation und Kürettage
(D&C) oder Patienten-Timing). Patientinnen, die nach dem Zufallsprinzip
dem Kontrollarm der zweigleisigen Studie zugewiesen wurden, unterzogen
sich als Endometrium-Vorbehandlung der Schlingenresektion.
Studienendpunkte: Als primärer Maßstab der Wirksamkeit wurde ein
validiertes Menstruationstagebuch-Wertesystem gewählt, das von Higham
(Higham JM, O'Brien PMS, Shaw RW Br J Obstet Gynaecol 1990; 97:734-
9) entwickelt wurde. Die Einschätzung des Menstruationsblutverlustes
erfolgte anhand eines Schaubildes zur Blutverlusteinschätzung
(Pictorial Blood Loss Assessment Chart, PBLAC). Als Patientenerfolg
wurde eine Reduktion des Menstruationsflusses ein Jahr nach dem
Verfahren auf einen Tagebuchwert von <75definiert. Als Studienerfolg
wurde ein statistischer Unterschied von weniger als 20 % in den
Patientenerfolgsraten zwischen dem NovaSure impedanzgesteuerten
Endometrium-Ablationssystem und der Schlingenresektion plus
Rollerball-Ablation definiert. Die Patientinnen wurden nach zwei und
nach dreiJahren kontaktiert und um die Beantwortung einer Reihe von
Fragen zu ihren Blutungen in den letzten 12Monaten gebeten. Es wurde
der Menstruationsblutungsstatus jeder Patientin nach zwei und drei
Jahren bestimmt, wobei der Wert nach einem Jahr im Schaubild zur
Blutverlusteinschätzung (PBLAC) und das Blutungsmuster als Referenz
dienten. Auf diese Weise war es möglich, das Blutungsmuster oder den
Menstruationsstatus einer Patientin nach einem Jahr direkt mit dem
Blutungsmuster nach zwei und drei Jahren zu vergleichen.
Sekundäre Endpunkte lieferten die angewandte Anästhesie, die Länge
des Verfahrens und Antworten auf eine Befragung zur Lebensqualität.
Die Sicherheit wurde anhand der während der Studie gemeldeten
Nebenwirkungen beurteilt.
Methoden: Eine zufallsgesteuerte (2:1), prospektive klinische Studie wurde
an 9 klinischen Standorten durchgeführt und umfasste 265 Patientinnen,
die zuvor mit Menorrhagie diagnostiziert worden waren. Präoperativ sowie
einmal monatlich 12Monate lang nach dem Verfahren wurden Werte
in einem Menstruationstagebuch gesammelt. Die Patientinnen wurden
zu einem beliebigen Zeitpunkt während ihres Zyklus behandelt. Keine
der Patientinnen erhielt eine hormonelle Vorbehandlung zum Abbau der
Endometrium-Zellschicht. Bei den Patientinnen in der Kontrollgruppe
wurde eine hysteroskopische Schlingenresektion des Endometriums als
mechanische Methode zur Endometrium-Vorbehandlung vorgenommen,
gefolgt von der Rollerball-Ablation. Die Studienteilnehmerinnen mussten die
folgenden Schlüsselkriterien zur Patientenauswahl erfüllen:
Einschlusskriterien
• Hartnäckige Menorrhagie ohne definierbare organische Ursache
(dysfunktionelle Uterusblutung)
• Alter 25 bis 50Jahre
• Uterus-Ultraschallmessung von 6,0–10,0cm (äußerer Muttermund bis
interner Fundus)

8
DEUTSCH
• 3Monate vor Studienbeginn einen Mindestwert von >150 im Schaubild
zur Blutverlusteinschätzung (PBLAC) oder einen Monat lang einen Wert
von >150 im PBLAC bei Frauen:
- die seit mindestens 3 Monaten (dokumentiert) erfolglos medizinisch
therapiert wurden;
- bei denen eine medizinische Behandlung kontraindiziert war oder
- die eine medizinische Behandlung abgelehnt haben.
Ausschlusskriterien
• Vorliegen von Bakteriämie, Sepsis oder einer anderen aktiven
systemischen Infektion
• Akute oder wiederkehrende chronische Beckenentzündung
• Patientinnen, die an dokumentierten Koagulopathien leiden oder
Antikoagulanzien einnehmen
• Symptomatische Endometriose
• Frühere Operation am Uterus (außer Kaiserschnitt im unteren Segment),
durch die die Uteruswand ihre ursprüngliche Beschaffenheit verloren hat,
z. B. transmurale Myomektomie oder klassischer Kaiserschnitt
• Frühere Endometriumablation
• Patientinnen, die Medikamente einnehmen, die zu einem Abbau des
myometrialen Muskels führen könnten, wie z. B. Steroideinnahme über
einen längeren Zeitraum
• Patientinnen, die noch einen Kinderwunsch haben oder ihre
Fruchtbarkeit erhalten möchten
• Patientinnen, die derzeit hormonelle Verhütungsmittel einnehmen oder
nicht willens sind, nach der Ablation nichthormonale Verhütungsmethoden
anzuwenden
• Durch Hysteroskopie, SIS (saline infusion sonohysterography,
Hysterographie mit Kochsalzinfusion) oder HSG (Hysterosalpingographie)
bestätigte abnorme/blockierte Uterushöhle. Speziell:
- Uterus septus oder bicornis oder eine andere angeborene Missbildung
der Uterushöhle
- gestielte, submuköse oder andere Leiomyome, durch die die
Uterushöhle entstellt wird; Polypen (größer als 2cm), durch die die
Menorrhagie der Patientin wahrscheinlich verursacht wird
- vorhandenes Intrauterinpessar (IUD)
• Vermutete oder nachgewiesene bösartige Erkrankung des Uterus
innerhalb der letzten fünf Jahre, die durch Histologie bestätigt wurde
• Durch Histologie bestätigte Endometrium-Hyperplasie
• Unbehandelte Zervixdysplasie
• Erhöhte FSH-Werte, die mit einer Ovarialinsuffizienz übereinstimmen
(>40IU/ml)
• Schwangerschaft
• Akute Geschlechtskrankheit
Patientenpopulation: An dieser Studie nahmen insgesamt
265Patientinnen teil. Das Alter der Patientinnen lag zwischen 25 bis
50 Jahren, wobei 46 % unter 40 und 54 % 40Jahre oder älter waren.
Zwischen den Behandlungsgruppen, den Altersgruppierungen oder den
neun Untersuchungsstandorten lagen keine demografischen Unterschiede
oder unterschiedlichen Parameter der gynäkologischen Anamnese vor.
Tabelle 2. Patientennachweisbarkeit
Anzahl der Patientinnen NovaSure Schlingenresektion
plus Rollerball
Anzahl bei Studienbeginn
(Intent-to-Treat-Population) 175 90
Abgebrochene Verfahren*1–4 –2
Behandelt 171 88
Zusätzliche Behandlung* –4 –2
Hysterektomie*2–3 –2
Nicht für Nachuntersuchung verfügbar* –5 –2
Morbus Hodgkin* –1 0
Beckenschmerzen – Verabreichung
von Leuprolid*
–1 0
Verfügbare Daten bei
Nachuntersuchung
nach 12Monaten
157 82
Zusätzliche Behandlung* –2 –1
Hysterektomie*2–3 –1
Nicht für Nachuntersuchung verfügbar* –2 –5
Arzttermin nicht eingehalten –1 –1
Teilnahme abgelehnt* –1 0
Schwangerschaft* –1 0
Verfügbare Daten bei
Nachuntersuchung
nach 24Monaten
147 74
Zusätzliche Behandlung* 0 –4
Hysterektomie*2–5 –1
Nicht für Nachuntersuchung verfügbar* –4 –2
Nachuntersuchung nach 36 Monaten 138 67
Nicht für Nachuntersuchung nach
24 Monaten verfügbar, Teilnahme an
Nachuntersuchung nach 36 Monaten
+1 +1
Verfügbare Daten bei
Nachuntersuchung nach 36Monaten 139 68
* Ausgeschiedene Patientinnen
1 Vier NovaSure-Patientinnen erfüllten nicht die Protokoll-Einschlusskriterien; zwei Rollerball-Patientinnen
hatten eine Uterusperforation
2 Für Hysterektomie, siehe Tabelle 7
Ergebnisse
Primärer Wirksamkeitsendpunkt: Blutungswert
Als Patientenerfolg 12 Monate nach dem Eingriff wird eine Reduzierung
des Tagebuchwertes von >150 vor dem Eingriff auf <75 nach dem Eingriff
definiert. Amenorrhoe ist als Wert 0 definiert. Als Erfolg nach 24 und nach
36 Monaten, basierend auf Telefonbefragungen, wird eine Eliminierung der
Blutungen oder eine Reduzierung auf eine leichte oder normale Regelblutung
definiert. Die in Tabelle 3 (unten) dargelegten Daten repräsentieren die
klinischen Ergebnisse basierend auf der Gesamtzahl von 265 Patientinnen,
die nach dem Zufallsprinzip der Studie zugewiesen wurden (Intent-to-Treat-
Gruppe, ITT). Es wird vom Schlimmstfall-Szenario ausgegangen, wobei zur
Berechnung der in der Tabelle aufgeführten Werte jede der ausgeschiedenen
Patientinnen (Beschreibung in Tabelle 2 für Patientennachweisbarkeit) als
„Ausfall“ gezählt wird.

9
DEUTSCH
Tabelle 3. Wirksamkeit: Erfolgsraten–Intent-To-Treat-Patientinnen
NovaSure
(n=175)
Schlingenresektion
Plus Rollerball
(n=90)
Monate nach Ablation 12* 24** 36** 12* 24** 36**
Anzahl der erfolgreichen
Patientinnen 136 143 134 67 68 63
Studienerfolgsrate 77,7 % 81,7 % 76,6 % 74,4 % 75,6 % 70,0 %
Anzahl der Patientinnen
mit Amenorrhoe 63 64 58 29 26 23
Amenorrhoe-Rate 36,0 % 36,6 % 33,1 % 32,2 % 28,9 % 25,6 %
* Basierend auf Tagebuchwerten
** Basierend auf Telefonbefragungen
Sekundärer Wirksamkeitsendpunkt: Lebensqualität
Die Lebensqualität (Quality of Life, QOL) der Patientin wurde anhand
der Auswertung einer Befragung zur Lebensqualität (SF-12) und einer
Befragung zur Auswirkung der Menstruation vor der Behandlung und 3,
6, 12, 24 und 36Monate nach dem Verfahren beurteilt. Tabelle 4 zeigt
die Antworten der Patientinnen beider Gruppen vor dem Eingriff, sofern
zutreffend, und 12, 24 und 36Monate nach dem Verfahren.
Tabelle 4. Wirksamkeit: Lebensqualität (QOL)
NovaSure Schlingenresektion
plus Rollerball
Anzahl der die Befragung zur Lebensqualität beantwortenden Patientinnen
#
Präoperativ 175 90
12 Monate 154 82
24 Monate 143 73
36 Monate 139 67
Prozentsatz zufriedener oder sehr zufriedener Patientinnen
12 Monate 92,8 % 93,9 %
24 Monate 93,9 % 89,1 %
36 Monate 96,3 % 89,7 %
Prozentsatz der Patientinnen, die dieses Verfahren wahrscheinlich oder auf alle
Fälle weiterempfehlen würden
12 Monate 96,7 % 95,9 %
24 Monate 96,6 % 94,5 %
36 Monate 97,8 % 92,6 %
Prozentsatz der Patientinnen mit Dysemenorrhoe
Präoperativ 57,1 % 55,6 %
12 Monate 20,8 %& 34,2 %*,&
24 Monate 20,3 %* 30,1 %*
36 Monate 17,3 %* 28,4 %*
Prozentsatz der Patientinnen mit PMS
Präoperativ 65,1 % 66,7 %
12 Monate 36,4 %* 35,4 %*
24 Monate 44,0 %* 46,6 %*
36 Monate 34,5 %* 41,2 %*
Prozentsatz der Patientinnen, die von gelegentlichen, häufigen oder ständigen
Schwierigkeiten bei der Ausübung ihrer beruflichen Tätigkeit oder anderer
Aktivitäten aufgrund der Menstruation berichten
Präoperativ 66,3 % 65,5 %
12 Monate 9,9 %* 8,6 %*
24 Monate 14,5 %* 15,0 %*
36 Monate 16,3 %* 13,3 %*
Prozentsatz der Patientinnen, die von gelegentlichen, häufigen oder ständigen
Sorgen aufgrund der Menstruation berichten
Tabelle 4. Wirksamkeit: Lebensqualität (QOL)
NovaSure Schlingenresektion
plus Rollerball
Präoperativ 74,7 % 68,9 %
12 Monate 23,6 %* 18,5 %*
24 Monate 24,2 %* 19,2 %*
36 Monate 18,7 %* 19,1 %*
Prozentsatz der Patientinnen, die von gelegentlich, häufig oder ständig aufgrund
der Menstruation verpassten gesellschaftlichen Aktivitäten berichten
Präoperativ 63,3 % 62,2 %
12 Monate 8,5 %* 8,6 %*
24 Monate 9,0 %* 11,1 %*
36 Monate 8,1 %* 10,8 %*
# Nicht alle Patientinnen haben an der Befragung teilgenommen
* Statistisch signifikanter Unterschied gegenüber präoperativer Antwort (Chi-Quadrat; p<0,05)
& Statistisch signifikanter Unterschied zwischen NovaSure- und Rollerball-Gruppen (Chi-Quadrat; p=0,02)
Sicherheitsendpunkt
Informationen zu Nebenwirkungen sind in diesem Handbuch im Abschnitt
„Nebenwirkungen“ zu finden.
Sekundärer Endpunkt: Verfahrensdauer
Die Verfahrensdauer, ein sekundärer Endpunkt, wurde für jede Patientin
bestimmt, indem der Zeitpunkt der Instrumenteneinführung und die
Zeit der Instrumentenentnahme festgehalten wurde. Die mittlere
Verfahrensdauer war bei den NovaSure-Patientinnen bedeutend kürzer als
die Verfahrensdauer der Rollerball-Gruppe (4,2 ± 3,5 Minuten gegenüber
24,2 ± 11,4 Minuten). Die mittlere Dauer für die Anwendung von HF-
Energie betrug in einem Teilsatz überwachter NovaSure-Patientinnen 84,0
± 25,0 Sekunden (Tabelle5).
Tabelle 5. Operative Verfahrensdauer
Operative Parameter NovaSure
n=175
Schlingenresektion
plus Rollerball
n=90
Anzahl der behandelten Patientinnen* 171 88
Verfahrensdauer in Minuten (± SD)
(Einführung bis Herausnahme des
Instruments)
4,2 ± 3,5** 24,2 ± 11,4**
Verfahrensdauer in Sekunden (± SD)
(Zeitdauer der Energieabgabe)
84,0 ± 25,0 n.f.#
* Siehe Tabelle 2 zur Patientennachweisbarkeit
** Statistisch signifikanter Unterschied zwischen Behandlungsgruppen (Student-t-Test; p <0,05)
# nicht festgestellt
Sekundärer Endpunkt: angewandte Anästhesie
Die Verabreichung eines Anästhetikums lag im Ermessen jeder Patientin,
des Studienleiters und des anwesenden Anästhesisten. Bei 27,0 % (47/174)
der NovaSure-Patientinnen wurde das Verfahren unter Vollnarkose oder
Epiduralanästhesie und bei 73,0 % (127/174) unter örtlicher Betäubung bzw.
mit einem intravenös verabreichten Beruhigungsmittel durchgeführt. Bei
einer Patientin in dieser Gruppe wurden keine Angaben zur angewandten
Anästhesie gemacht. 82,2 % (74/90) der Patientinnen in der Rollerball-
Gruppe wurden unter Vollnarkose oder Epiduralanästhesie behandelt
und 17,8 % (16/90) unter örtlicher Betäubung bzw. mit einem intravenös
verabreichten Beruhigungsmittel (Tabelle 6).

10
DEUTSCH
einer Schwangerschaft nach dem Verfahren erheblich geringer ist.
Gebärfähige Patientinnen sollten vor potenziellen Komplikationen
gewarnt werden, die im Falle einer Schwangerschaft auftreten könnten.
Diese Beratung sollte, sofern angebracht, auf eine nach dem Verfahren
erforderliche Empfängnisverhütung eingehen. Dieses Verfahren ist keine
Sterilisationsmethode und spätere Schwangerschaften können für die
Mutter und für den Fetus gefährlich sein.
Während der ersten Wochen nach der Ablation ist in der Regel
Scheidenausfluss zu beobachten, der bis zu einem Monat andauern
kann. Der Ausfluss wird in den ersten Tagen im Allgemeinen als blutig,
nach ungefähr einer Woche als blutig-seriös und danach als reichlich
und wässrig beschrieben. Ein ungewöhnlich oder faul riechender
Ausfluss sollte sofort dem Arzt mitgeteilt werden. Zu anderen üblichen
Komplikationen nach dem Verfahren gehören Krämpfe/Beckenschmerzen,
Übelkeit und Erbrechen.
In der Differentialdiagnose einer postoperativen Patientin, die über akute
Unterleibsschmerzen, Fieber, Kurzatmigkeit, Schwindel, Hypotonie oder
andere Symptome klagt, die mit einer Uterusperforation mit oder ohne
Schädigung der angrenzenden Organe der Bauchhöhle einhergehen
können, sollte eine Uterusperforation in Betracht gezogen werden.
DiePatientinnen müssen in der Beratung dazu angehalten werden,
solche Symptome unverzüglich ihrem Arzt mitzuteilen.
Vorbereitung der Patientin auf die Behandlung
Das NovaSure Impedanzgesteuerte Endometrium-Ablationssystem kann
eine Uterushöhle erfolgreich über einen Bereich unterschiedlich dicker
Endometrium-Zellschichten behandeln. Die Uterusschleimhaut muss
vor dem Verfahren nicht abgetragen werden und das Verfahren kann
während der proliferativen oder der sekretorischen Phase des Zyklus
vorgenommen werden. Die Sicherheit und Wirksamkeit des NovaSure-
Systems wurde bei Patientinnen mit medikamentöser oder chirurgischer
Vorbehandlung zwar noch nicht vollständig beurteilt, es liegen jedoch
Daten von einer begrenzten Anzahl von Patientinnen vor, die ohne
Komplikationen oder nachteilige Auswirkungen mit GnRH-Agonisten
vorbehandelt wurden.
Es hat sich erwiesen, dass eine akute Blutung kein einschränkender
Faktor bei der Verwendung des NovaSure-Systems ist. Es wird
empfohlen, dass mindestens eine Stunde vor der Behandlung und
danach postoperativ ein nichtsteroidales entzündungshemmendes
Medikament (NSAID) verabreicht wird, um das Auftreten intraoperativer
und postoperativer Uteruskrämpfe zu reduzieren.
Tabelle 6. Angewandte Anästhesie
NovaSure
n=175*
Schlingenresektion
plus Rollerball
n=90
Vollnarkose oder Epiduralanästhesie 27,0 % 82,2 %
Örtliche Betäubung und/oder intravenös
verabreichtes Beruhigungsmittel 73,0 % 17,8 %
* Bei einer Patientin wurden keine Angaben zur angewandten Anästhesie gemacht.
Klinische Beobachtungen
Hysterektomie
Fünfzehn Frauen unterzogen sich innerhalb von drei Jahren nach dem
Ablationsverfahren einer Hysterektomie. Tabelle 7 listet die Gründe für die
Hysterektomie auf.
Tabelle 7. Hysterektomie
Grund für die Hysterektomie NovaSure
n=175
Schlingenresektion
plus Rollerball
n=90
Diagnostiziertes Adenokarzinom zum
Zeitpunkt des Ablationsverfahrens 1 1
Fibrome 2 0
Beckenabszess 1 1
Endometriose 3 0
Adenomyose 4 0
Hämatometra 0 1
Menorrhagie 0 1
INSGESAMT 11 (6,3 %) 4 (4,4 %)
7 Hysterektomien wurden bei Patientinnen <40 Jahre (7 NovaSure) und 8 Hysterektomien wurden bei Patienten
>40 Jahre (4 NovaSure, 4 Rollerball) vorgenommen.
Patientenauswahl
Menorrhagie kann durch eine Vielzahl zugrunde liegender Probleme
verursacht werden, u. a. Endometriumkarzinom, Myome, Polypen,
Medikamente und dysfunktionelle Uterusblutung (anovulatorische
Blutung). Patientinnen sollten immer untersucht und beurteilt werden,
um die Ursache für die starke Uterusblutung zu bestimmen, bevor
eine mögliche Behandlung eingeleitet wird. Vor Durchführen eines
Endometrium-Ablationsverfahrens sollte die medizinische Fachliteratur
zu unterschiedlichen Endometrium-Ablationstechniken, Indikationen,
Kontraindikationen, Komplikationen und Gefahren zu Rate gezogen werden.
Patientenberatung
Wie bei jedem anderen Verfahren muss der Arzt die Risiken,
Vorteile und Alternativen mit der Patientin besprechen, bevor eine
Endometriumablation durchgeführt wird. Die Erwartungen der Patientin
sollten so angesetzt werden, dass sich diese darüber im Klaren ist,
dass es das Ziel der Behandlung ist, die Blutung auf eine normale
Regelblutung zu reduzieren.
Das Einmalinstrument ist nur zur Verwendung bei Frauen bestimmt,
die keinen Kinderwunsch mehr hegen, da die Wahrscheinlichkeit

11
DEUTSCH
NovaSure Impedanzgesteuertes Endometrium-
Ablationssystem – Bedienungsanleitung
Vor der Verwendung bitte alle Anweisungen, Vorsichtsmaßnahmen und
Warnhinweise lesen.
1.0 Einrichtung
NovaSure
HF-CONTROLLER
NovaSure EINMALINSTRUMENT
MIT VERBINDUNGSKABEL,
INKL. TROCKENMITTELFILTER
FÜR ABSAUGLEITUNG
NovaSure NETZKABEL NOVASURE TROCKENMITTELFILTER
FÜR ABSAUGLEITUNG
NovaSure FUSSSCHALTER NovaSure CO2-KANISTER
1.1 Bei der Verwendung des NovaSure-Systems werden die folgenden
Artikel benötigt:
• ein steriles, für die Verwendung bei nur einer Patientin bestimmtes
NovaSure-Einmalinstrument mit
• Verbindungskabel
• ein NovaSure HF-Controller
• ein NovaSure-Fußschalter
• ein NovaSure-Wechselstromkabel
• ein unsteriler Trockenmittelfilter für die NovaSure-Absaugleitung
• ein NovaSure CO2-Kanister
Vakuum-
sicherheitsventil
Zervixmanschette
Bipolares
Elektroden-
array
Vorderer Griff
Hülse
Hinterer
Griff
Absaug-
leitung
Entriegelungs-
knopf
Einstellen der Länge der Uterushöhle
Schlauchtülle
der Vakuum-
Rückführungsleitung
WIDTH
(Breitenskala)
Hinweis: Es sollten mindestens ein zusätzliches Einmalinstrument,
ein zusätzlicher Trockenmittelfilter und ein zusätzlicher CO2-
Kanister zur Hand sein.
1.2 Den NovaSure HF-Controller vorbereiten. Auf einen kleinen
Tisch neben der Patientin und im Blickfeld des Chirurgen legen.
Das Wechselstromkabel an den Controller und eine Steckdose
anschließen.
1.3 Den CO2-Kanister in den Regler an der Rückseite des Controllers
einschrauben, bis er fest sitzt.
1.4 Den CO2-Reglerknopf vollständig in die HI-Position drehen
(fallsvorhanden).
Hinweis: Bei neueren Controller-Modellen befindet sich kein Knopf am
Regler, da der CO2-Fluss automatisch reguliert wird. Falls der Controller
nicht über einen Reglerknopf verfügt, mit Schritt 1.5 fortfahren.
1.5 Den Kippschalter an der Rückwand des Controllers in die Position „on“
drücken.
1.6 Den Fußschalter an den entsprechenden Anschluss an der Vorderseite
des Controllers anschließen.
Anschluss
Hinweis: Wenn der HF-Controller, Modell 10 zum ersten Mal
eingeschaltet wird, wird der Bildschirm „Sprache auswählen“
angezeigt. Die Standardeinstellung ist Englisch. Um eine andere
Sprache auszuwählen, die Schaltfläche mit dem Namen der
gewünschten Sprache drücken. Die Auswahl durch Drücken der grün
blinkenden Schaltfläche speichern.
Die Sprachauswahl wird gespeichert. Die Sprachauswahl kann
nach der ursprünglichen Einrichtung mithilfe des Bildschirms
„Einstellungen“ geändert werden. Um die in der Bildschirmanzeige
verwendete Sprache zu ändern, den Namen der betreffenden Sprache
drücken. Zum Speichern von Änderungen an den Einstellungen die
grün blinkende Schaltfläche drücken. ZumAbbruch einer Auswahl
auf das blaue „X“ drücken.
Kipp-
schalter
CO2-Kanister
Wechselstromkabel

12
DEUTSCH
Hinweis: Bei Patientinnen, bei denen die Uterushöhle länger als
6,0 cm ist, lagen die zu beobachtenden Erfolgsraten unter den
Gesamterfolgsraten der Studie.
2.11 Die sterile Verpackung des NovaSure-Einmalinstruments
öffnen. Das Einmalinstrument mit dem Verbindungskabel in das
sterile Feld legen und dabei darauf achten, dass die unsterile
Trockenmittelfilterpackung für die Absaugleitung vom sterilen Feld
ferngehalten wird.
Warnung: Das sterile, zur Verwendung bei nur einer Patientin
bestimmte Einmalinstrument darf nicht verwendet werden, wenn
die Verpackung beschädigt zu sein scheint oder Anzeichen einer
Manipulation aufweist.
2.12 Die unsterile Packung und den Beutel des Trockenmittelfilters für
die Absaugleitung öffnen. Die roten Kappen abnehmen.
Vorsicht: Der Trockenmittelfilter der Absaugleitung ist unsteril.
Die Verpackung sollte nicht ins sterile Feld gelegt werden.
Vorsicht: Weist das Trockenmittel der Absaugleitung eine rosa
Farbe auf, muss der Filter vor Beginn des Ablationsverfahrens
ersetzt werden.
2.13 Den Trockenmittelfilter an die Schlauchtülle am Absaugschlauch
des Einmalinstruments anschließen. Darauf achten, dass die Rillen
der Schlauchtülle vollständig in den Schlauch am Trockenmittelfilter
eingeführt sind.
2.14 Vorsicht: Das Einmalinstrument muss sich außerhalb der
Patientin befinden, bevor Schritt 2.15 durchgeführt wird.
2.15 Das Kabel des Einmalinstruments an den entsprechenden
Anschluss an der Vorderseite des Controllers anschließen.
Einmalinstrument-
Anschluss
2.0 Verfahren
2.1 Die Patientin auf die Narkose vorbereiten.
2.2 Die Patientin in die Steinschnittlage bringen.
2.3 Gemäß Standardverfahren eine Narkose verabreichen.
2.4 Eine bimanuelle Untersuchung durchführen. Auf schwere
Anteversion oder Retroversion prüfen.
2.5 Patientin ähnlich wie bei einer Dilatation und Kürettage (D&C)
vorbereiten und mit Tüchern abdecken.
2.6 Ein Spekulum in die Scheide einführen.
2.7 Die Zervix mit einem Tenaculum fassen.
2.8 Eine Ultraschallmessung des Uterus durchführen, um die Länge
vom Fundus bis zum externen Muttermund zu bestimmen.
DieWirksamkeit des NovaSure-Systems wurde bei Patientinnen
mit einer Uterus-Ultraschallmessung von mehr als 10 cm noch
nicht vollständig beurteilt.
2.9 Die Länge des Uterushalskanals bestimmen und den Kanal für
die Einführung des Instruments erweitern.
HINWEIS: Der Nenndurchmesser des NovaSure-Einmalinstrument
beträgt 6 mm.
2.10 Auf die betreffenden Uterustiefen- und Uterushalskanalmessungen
in der Tabelle zur Länge der Uterushöhle (s. unten) Bezug nehmen,
um die angemessenen Uteruslängeneinstellungen zu erhalten. Am
oberen Ende der Tabelle wurden die Abmessungen entsprechend
der Elektrodenlänge des Einmalinstruments angepasst.
Für eine sichere und effektive Behandlung ist es wichtig, dass
die Länge der Uterushöhle richtig bestimmt wird. Wenn die Länge
der Uterushöhle überschätzt wird, kann dies zu einer thermischen
Verletzung des Uterushalskanals führen.
Warnung: Bei der Sondierung, Dilatation oder Einführung des
Einmalinstruments ist Vorsicht geboten, damit die Uteruswand
nicht perforiert wird.
TABELLE 8. LÄNGE DER UTERUSHÖHLE
Uterus-Ultraschallmessung (cm)
Zervix-
länge (cm) 10 9,5 9 8,5 8 7,5 7 6,5 6
26,5* 6,5* 6,5* 6,5 6 5,5 5 4,5 4
2,5 6,5* 6,5* 6,5 6 5,5 5 4,5 4
36,5* 6,5 6 5,5 5 4,5 4
3,5 6,5 6 5,5 5 4,5 4
46 5,5 5 4,5 4
4,5 5,5 5 4,5 4
55 4,5 4
5,5 4,5 4
64
* Der Wert 6,5 soll nicht die numerische Differenz zwischen der Ultraschallmessung der Länge und
der Länge des Uterushalskanals wiedergeben.
Vielmehr wurde der Wert 6,5 angegeben, da er die maximale Länge darstellt, auf die die NovaSure-
Elektrode ausgefahren werden kann.
Kontraindikation: Patientinnen, deren Uterushöhle kürzer als 4cm
ist, dürfen nicht behandelt werden, da dies zu einer Verletzung des
Uterushalskanals führen könnte.

13
DEUTSCH
Warnung: Wenn das NovaSure-Einmalinstrument an den NovaSure
HF-Controller angeschlossen wird, startet der CO2-Fluss zum
Entlüften des Einmalinstruments und der Schläuche. Während
dieser Entlüftung, die ca. 10 Sekunden dauert, muss sich das
Einmalinstrument außerhalb der Patientin befinden. Auf der HF-
Steuereinheit Modell 10 wird eine Spülgerätemeldung angezeigt
und während des gesamten Bereinigungsvorgangs ertönt ein
hörbarer pulsierender Ton. Wenn der Ton verstummt und die LED/
Bildschirmmeldung erlischt, kann das NovaSure-Einmalinstrument
ohne Bedenken eingeführt werden.
Vorsicht: Vom Anschluss des Einmalinstruments an den Controller
bis zum Abschluss des Uterushöhlen-Beschaffenheitstests strömt
ununterbrochen CO2 aus. Um die Dauer der CO2-Abgabe und eine
mögliche Emboliegefahr so gering wie möglich zu halten, das
Einsetzverfahren sofort nach dem Einführen des Einmalinstruments
durchführen und direkt mit dem Perforationstest fortfahren.
Warnung: Bei der Sondierung, Dilatation oder Einführung des
Einmalinstruments ist Vorsicht geboten, damit die Uteruswand
nicht perforiert wird.
2.16 Stellen Sie das Einweggerät außerhalb des Patienten bereit und
stellen Sie sicher, dass die Bildschirmmeldung nicht auf der HF-
Steuereinheit Modell 10 angezeigt wird, wenn das Array geöffnet
wird. Wenn die Bildschirmmeldung weiterhin auf der HF-Steuereinheit
Modell 10 angezeigt wird, schließen Sie das Einweggerät und öffnen
Sie es erneut. Wenn sich das Problem dadurch nicht beheben lässt,
das Einmalinstrument austauschen.
2.17 Darauf achten, dass der auf der Breitenskala (WIDTH) angegebene
Wert größer als oder gleich 4,0 cm ist.
WIDTH
(Breitenskala)
Hinweis: Liegt der Wert auf der Breitenskala (WIDTH) unter 4,0 cm,
das Einmalinstrument schließen und Schritt 2.16 oben wiederholen.
Liegt der Wert auf der Breitenskala (WIDTH) weiterhin unter 4,0 cm,
ein neues Einmalinstrument öffnen und das defekte Einmalinstrument
an den technischen Kundendienst von Hologic zurücksenden.
2.18 Das Einmalinstrument entsperren, dazu den Entriegelungsknopf
drücken. Das Einmalinstrument schließen. Dazu den vorderen Griff
stationär halten und die hinteren Griffe vorsichtig zurückziehen,
bisder Indikator „ARRAY CLOSED“ für die geschlossene Elektrode
zu sehen ist, der sich am Gelenkteil zwischen dem vorderen
und hinteren Griffstück befindet. Daran ist zu erkennen, dass die
Goldnetzelektrode in die Hülse zurückgezogen wurde und dass
sichdas Einmalinstrument in der geschlossenen Position befindet.
ARRAY
CLOSED
Indikator
Entriegelungsknopf
2.19 Das Array muss vollständig von der externen Hülse umgeben sein.
2.20 Überprüfen, ob der Wert auf der Breitenskala (WIDTH) ca. 0,5 cm
anzeigt.
2.21 Auf die betreffenden Uterustiefen- und Uterushalsmessungen in
der Tabelle zur Länge der Uterushöhle (s. oben) Bezug nehmen,
um wie in Schritt 2.10 oben beschrieben die angemessene
Uteruslängeneinstellung zu erhalten.
Kontraindikation: Patientinnen, deren Uterushöhle kürzer als 4cm
ist, dürfen nicht behandelt werden, da dies zu einer Verletzung des
Uterushalskanals führen könnte.
2.22 Unter Bezugnahme auf die Tabelle zur Länge der Uterushöhle in
Abschnitt 2.10 den als Länge ermittelten Wert durch Drücken der
Aufwärts-/Abwärtspfeile auf dem Eingabebildschirm des NovaSure
HF-Controllers auswählen.
2.23 Mit der entsprechenden Vorrichtung am Einmalinstrument den
oben ermittelten Wert als Länge der Uterushöhle einstellen und
das Instrument in dieser Einstellung arretieren. (Siehe Schritt 2.21).
Die Zervixmanschette muss vollständig in ihre proximale Position
zurückgezogen sein.
2.24 Bestätigen Sie, dass die Cervix eine Ausdehnung von mindestens
6 mm aufweist (Nenndurchmesser des NovaSure Einweginstruments).
2.25 Einen leichten Zug auf das Tenaculum ausüben, um den Winkel des
Uterus so gering wie möglich zu halten.
2.26 Das Einmalinstrument so abwinkeln, dass es sich auf einer Linie mit
der Achse des Uterus befindet, während es durch den Uterushals in
die Uterushöhle eingeführt wird. Das Einmalinstrument vorschieben,
während der vordere Griff stationär gehalten wird, bis das distale
Ende der Hülse den Fundus berührt.

14
DEUTSCH
#10
Warnung: Wenn sich das Einmalinstrument nicht leicht in den
Uterushalskanal einführen lässt, muss unter Anwendung von
klinischem Sachverstand entschieden werden, ob er stärker
erweitert werden muss.
2.27 Das Einmalinstrument um ca. 0,5 cm aus dem Fundus zurückziehen.
Die Griffe langsam zusammendrücken (NICHT VERRIEGELN), bis
stärkerer Widerstand zu spüren ist.
Auf der Breitenskala (WIDTH) sollte ca. 0,5cm angezeigt werden.
An dieser Stelle wurde die externe Hülse zurückgezogen.
2.28 Die Griffe des Einmalinstruments weiter langsam zusammendrücken
und dabei das Einmalinstrument behutsam ~0,5 cm zum Fundus hin
und vom Fundus weg bewegen und den Griff des Einmalinstruments
45° gegen den Uhrzeigersinn von der vertikalen Ebene und 45° im
Uhrzeigersinn von der vertikalen Ebene drehen, bis sich die Griffe
verriegeln.
Der Wert auf der Breitenskala (WIDTH) sollte nun über 2,5cm
liegen.
Hinweis: Nachdem sich die Griffe des Einmalinstruments verriegelt
haben, sollte sich der Uterus zusammen mit dem Einmalinstrument
bewegen.
2.29 Das Einmalinstrument behutsam mit anterioren, posterioren und
lateralen Bewegungen bewegen.
2.30 Zum Abschluss des Einsetzens das Einmalinstrument leicht
zurückziehen, bis sich der Wert auf der Breitenskala (WIDTH)
umca.0,2–0,5 cm verringert.
0,5 cm

15
DEUTSCH
2.31 Das Tenaculum halten, das Einmalinstrument langsam und vorsichtig
bis zum Fundus vorschieben. Der Wert auf der Breitenskala (WIDTH)
sollte mindestens so groß wie die vorherige Messung sein.
2.32 Die Zervixmanschette nach vorne schieben. Dazu sanften Druck auf
die Lasche an der Zervixmanschette ausüben, bis diese mit dem
äußeren Muttermund abschließt.
2.33 Die Cornu-zu-Cornu-Messung (mindestens 2,5 cm) auf der
Breitenskala (WIDTH) ablesen.
Kontraindikation: Patientinnen, deren Uterushöhle weniger als
2,5cm breit ist, nicht behandeln. Dies lässt sich anhand der
Breitenskala (WIDTH) des Einmalinstruments nach Einsetzen des
Instruments feststellen.
Vorsicht: Sollte die Warnung „POSITION ELEKTRODE“ angezeigt
werden, im Abschnitt zur Fehlerbehebung unter „POSITION
ELEKTRODE-Alarm“ nachschlagen.
2.34 Den auf der Breitenskala (WIDTH) angegebenen Wert durch
Drücken der Aufwärts-/Abwärtspfeile auf dem Eingabebildschirm
des NovaSure HF-Controllers auswählen.
2.35 Das System kann entweder im automatischen oder im manuellen
Modus betrieben werden. Im automatischen Modus beginnt der
Ablationszyklus bei erfolgreichem Abschluss des Perforationstests
automatisch. Im manuellen Modus beginnt der Ablationszyklus nach
einem erfolgreichen Perforationstest nicht automatisch.
Hinweis: Das korrekte Einsetzen der Goldnetzelektrode am Fundus ist für eine sichere und effektive Behandlung wichtig. Wenn sich ein
Teil der Goldnetzelektrode oder der distale Rand der externen Hülse während der Behandlung im Uterushalskanal befindet, besteht ein
erhöhtes Risiko einer thermischen Verletzung des Uterushalses.
Fundus
Goldnetzelektrode
Hülsenrand
Uterushalskanal
Hülsenrand befindet sich
im unteren Uterussegment
Goldnetzelektrode
Uterushalskanal Hülsenrand
Hülsenrand befindet sich
im Uterushalskanal
Fundus
INKORREKTE POSITIONIERUNG KORREKTE POSITIONIERUNG
Geringer Druck
Fester Druck

16
DEUTSCH
Betrieb des HF-Controllers, Modell 10
A. Automatischer Modus
Um den HF-Controller, Modell 10 im automatischen Modus in
Betrieb zu nehmen, auf die Moduswechseltaste drücken, wenn
diese am unteren Bildschirmrand angezeigt wird. Mit Schritt
2.36 fortfahren, aber nicht Schritt 2.37 befolgen, wenn das
System im automatischen Modus betrieben wird.
B. Manueller Modus
Hinweis: Der manuelle Modus ist der standardmäßige Betrieb
des Systems.
Um das System im manuellen Modus in Betrieb zu nehmen,
nicht auf die Moduswechseltaste drücken, bevor mit dem
Perforationstest begonnen wird. Schritte 2.36 und 2.37
befolgen.
2.36 Durch einmalige Betätigung des Fußschalters den
Perforationstest starten. Auf dem Bildschirm wird
„Perforationstest läuft“ angezeigt, während nacheinander fünf
Punkte aufleuchten und erlöschen. Die Dauer des Tests beträgt
ca. zwischen 7 und 30Sekunden. Wenn der Perforationstest
erfolgreich war, wird der Bildschirm „Perforationstest
abgeschlossen“ angezeigt, und das System kann nun HF-
Energie abgeben. Das Einmalinstrument kann erst dann mit
Strom versorgt werden, wenn der Bildschirm „Perforationstest
abgeschlossen“ angezeigt wird.
Wenn der Perforationstest fehlschlägt, wird der Bildschirm
„Perforationstest erfolglos“ mit Schritten zur Fehlerbehebung
angezeigt.
A. Wenn Verdacht auf eine Perforation besteht, sollte das
Verfahren unverzüglich abgebrochen werden.
B. Sollte der Perforationstest erneut fehlschlagen, das System
und die Stelle zwischen der Zervix und der Zervixmanschette
auf Lecks überprüfen. Alle Schlauchanschlüsse überprüfen
und gewährleisten, dass ein Trockenmittelfilter für die
Absaugleitung installiert wurde. Bei einem Leck an der Zervix,
das sich nicht mithilfe der Zervixmanschette beheben lässt,
die Zervix um die Hülse herum mit einem anderen Tenaculum
fassen. Durch Betätigen des Fußschalters den Perforationstest
wiederholen.
Hinweis: Bei einer stark erweiterten Zervix kann am externen
Muttermund CO2 austreten. Unter diesen Bedingungen kann
das CO2-Leck von sichtbaren Bläschen oder einem zischenden
Geräusch begleitet sein.
C. Wenn der Perforationstest nach einer angemessenen Anzahl
von Versuchen der Fehlerbehebung (Schritt 2.36) immer noch
fehlschlägt, muss das Verfahren abgebrochen werden.
Hinweis: Wurde das Einmalinstrument nach Abschluss eines
Perforationstests aus der Uterushöhle entfernt, muss ein weiterer
Perforationstest durchgeführt werden, wenn das Einmalinstrument
wieder eingeführt wird (egal, ob der erste Test erfolgreich war oder
nicht), bevor mit einer Ablation begonnen wird.
2.37 Nur manueller Modus
Wird das System im manuellen Modus in Betrieb genommen, wird der
Ablationszyklus nach erfolgreichem Abschluss des Perforationstests
nicht automatisch gestartet. Sobald ein Perforationstest erfolgreich
abgeschlossen wurde, die Taste ENABLE (Aktivierung) drücken und
den Fußschalter ein zweites Mal betätigen, um den Ablationszyklus
zustarten.
Hinweis: Bei allen Modell-10-Geräten des HF-Controllers erfolgt eine
Vakuum-Vorprüfung vor Beginn des Ablationszyklus automatisch.
Der Bildschirm „Vakuumprüfung läuft“ wird angezeigt und ein
Signalton ist bis zu 10Sekunden lang während der Vakuum-
Vorprüfung zu hören.
Während des Ablationszyklus wird der Bildschirm „HF EIN“ mit
einem Timer angezeigt, der die Dauer der Ablation überwacht.
Hinweis: Die HF-Energieabgabe kann jederzeit durch Drücken des
Fußschalters gestoppt werden.
2.38 Nachdem der Ablationszyklus (nach ca. 90Sekunden) automatisch
beendet wurde, die Manschette mithilfe der Lasche an der
Zervixmanschette vollständig in ihre proximale Position zurückziehen.
VORSICHT: Die Zervixmanschette muss vollständig in ihre proximale
Position zurückgezogen sein, um eine mögliche Beschädigung der
Hülse beim Schließen der Elektrode zu minimieren.
Zervix-
manschette

17
DEUTSCH
Nach Abschluss des Ablationszyklus wird der Bildschirm „Ablation
abgeschlossen“ mit einer Zusammenfassung des Verfahrens angezeigt.
Der Bildschirm „Ablation abgeschlossen“ erfasst für jedes Verfahren die
folgenden Daten:
• Länge der Gebärmutterhöhle
• Breite der Gebärmutterhöhle
• Leistungsstufe
• HF-Ablationszeit
2.39 Das Einmalinstrument entsperren, dazu den Entriegelungsknopf
drücken. Das Einmalinstrument schließen. Dazu den vorderen Griff
stationär halten und die hinteren Griffe vorsichtig zurückziehen,
bis der Indikator „ARRAY CLOSED“ für die geschlossene Elektrode
zu sehen ist, der sich am Gelenkteil zwischen dem vorderen
und hinteren Griffstück befindet. Daran ist zu erkennen, dass die
Goldnetzelektrode in die Hülse zurückgezogen wurde und dass sich
das Einmalinstrument in der geschlossenen Position befindet.
Hinweis
: Falls es schwer ist, das Einmalinstrument zu schließen und
zu entfernen, siehe den Abschnitt zur Fehlerbehebung „Schwierigkeiten
beim Schließen und Entfernen des Einmalinstruments nach der Ablation“.
VORSICHT: Beim Zurückziehen der Elektrode vorsichtig vorgehen,
um das Gerät nicht zu beschädigen.
2.40 Das Einmalinstrument aus der Patientin entfernen.
2.41 DEN NOVASURE HF-CONTROLLER AUSSCHALTEN.
2.42 Die Patientin gemäß Standardverfahren postoperativ betreuen.
2.43 Die Patientin auf Veranlassung des behandelnden Arztes aus dem
Krankenhaus bzw. der Arztpraxis entlassen.
Regelmäßige Wartung und Reparatur
Die HF-Steuereinheit wurde speziell entwickelt und getestet, um IEC
60601-1 und andere Sicherheitsnormen zu erfüllen. Eine Wartung
ist nicht erforderlich, da das System beim Einschalten des Geräts
selbstständige Kontrollen durchführt. Zur Reinigung der Steuereinheit
siehe Abschnitt „Reinigung und Desinfektion“.
Die erwartete Lebensdauer der HF-Steuereinheit beträgt fünf Jahre oder
2000 Eingriffe, vorausgesetzt, dass Schäden durch Herunterfallen oder
grobe Handhabung vermieden werden. Wenn die Steuereinheit fallen
gelassen wird oder anderen schweren physikalischen Einwirkungen
ausgesetzt wird, beenden Sie die Verwendung und wenden Sie sich an
den technischen Kundendienst von Hologic.
Siehe Abschnitt „Informationen zum technischen Kundendienst und zur
Produktrückgabe“.
Für den NovaSure HF-Controller ist kein Reparaturhandbuch verfügbar,
da sich im Instrument keine vor Ort zu reparierenden Komponenten
befinden.
WARNUNG: Eine Modifikation dieses Geräts ist nicht gestattet.
Test der HF-Energieabgabe
Bei dem NovaSure HF-Controller, Modell 10 wurde im Einschalt-
Selbsttest (Power On Self Test, POST) ein automatischer Test der
Energieabgabe integriert. Während der POST-Sequenz wird die
Energieabgabe des Controllers (Pc) in einen Nebenschlusswiderstand
(Rs) innerhalb des Controllers geleitet. Der Zielwert für Pc ist 180 Watt,
und der Nennwert von Rs ist 25 Ohm. Während der POST-Sequenz wird
der Anschluss des Einmalinstruments vorne am Controller nicht mit
Strom versorgt.
Der NovaSure HF-Controller, Modell 10 führt die POST-Sequenz
automatisch beim Einschalten aus. Um auf die Daten der POST-Sequenz
zuzugreifen, unter „Einstellungen“ zu „System-Info“ scrollen. Auf die
Schaltfläche „Info anzeig.“ drücken.
Hinweis: Sollte während der POST-Sequenz ein Systemfehler
auftreten, den Netzschalter am Stromeingangsmodul ausschalten
und den Test wiederholen. Tritt der Systemfehler ein zweites Mal
auf, den HF-Controller außer Betrieb nehmen und den Hologic
Kundendienst benachrichtigen.
VORSICHT: Am Controller dürfen bei vermuteten Problemen keine
eigenmächtigen Reparaturen vorgenommen werden. Die Anleitung
zur Fehlerbehebung in diesem Handbuch befolgen. Sollten die
Probleme fortbestehen, den technischen Kundendienst von Hologic
telefonisch um Anweisungen bitten.
Steriles NovaSure-Einmalinstrument: Keine Wartung erforderlich.
Zur Verwendung bei nur einer Patientin bestimmt. Das NovaSure-
Einmalinstrument darf nicht wiederverwendet oder resterilisiert werden.

18
DEUTSCH
Bildschirmsymbole des NovaSure HF-Controllers, Modell 10
Es folgt eine Beschreibung der Symbole auf dem Bildschirm des
NovaSure HF-Controllers, Modell 10.
Symbol Einstellungen:
Zur Anzeige der Einstellungsoptionen
für Sprache, Helligkeit und Lautstärke
diese Schaltfläche drücken.
Symbol Letztes Verfahren:
Zur Anzeige des Bildschirms
„Ablation abgeschlossen“ und
Prüfung der Zusammenfassung
des letzten Verfahrens diese
Schaltfläche drücken.
Hilfe-Symbol:
Um weitere Informationen zum aktuellen Schritt des Verfahrens
anzuzeigen, diese Schaltfläche drücken. Unter diesem Symbol wird
eine Kurzfassung des Handbuchs angezeigt.
Hinweis: Wenn das Symbol „Last Procedure“ (Letztes Verfahren)
gedrückt wird, wird nur die vorherige Ablation angezeigt.
Informationen zu Verfahren, die vor dem jüngsten Verfahren
stattfanden, sind nicht verfügbar.
Hinweis: Auf dem Bildschirm „Einstellungen“ auf die Schaltfläche
„–“ oder „+“ drücken, um die Lautstärke und die Helligkeit
einzustellen.
Hinweis: Wenn der HF-Controller, Modell 10 zum ersten Mal
eingeschaltet wird, wird der Bildschirm „Sprache auswählen“
angezeigt. Die Standardeinstellung ist Englisch. Um eine andere
Sprache auszuwählen, die Schaltfläche mit dem Namen der
gewünschten Sprache drücken. Die Auswahl durch Drücken der
grün blinkenden Schaltfläche speichern. Die Sprachauswahl wird
gespeichert. Die Sprachauswahl kann nach der ursprünglichen
Einrichtung mithilfe des Bildschirms „Einstellungen“ geändert werden.
Um die in der Bildschirmanzeige verwendete Sprache zu ändern,
den Namen der betreffenden Sprache drücken. Zum Speichern von
Änderungen an den Einstellungen die grün blinkende Schaltfläche
drücken. Zum Abbruch einer Auswahl auf das blaue „X“ drücken.
Fehlerbehebung für die häufigsten Alarme
PERFORATIONSTEST-ALARM
Wenn der Perforationstest fehlschlägt, wird der Bildschirm
„Perforationstest erfolglos“ mit einer Kurzfassung der Tipps zur
Fehlerbehebung angezeigt. Der Grund für ein Fehlschlagen des
Perforationstests besteht darin, dass die Uterushöhle nicht unter Druck
gesetzt werden kann. Die Ursache dafür kann sein:
1. Leck am Instrument: Gewährleisten, dass der Trockenmittelfilter
für die Absaugleitung installiert wurde. Alle Schlauchanschlüsse
überprüfen, um zu gewährleisten, dass sie fest angeschlossen sind.
2. Leck am äußeren Muttermund: Auf sichtbare Bläschen oder ein
zischendes Geräusch am äußeren Muttermund untersuchen.
Die Zervixmanschette mithilfe der daran befindlichen Lasche in Richtung
des äußeren Muttermunds vorschieben, um zu gewährleisten, dass
diese eng mit dem äußeren Muttermund abschließt. Perforationstest
wiederholen. Sollte der Perforationstest erneut fehlschlagen, die Zervix
um die Hülse des NovaSure-Einmalinstruments herum mit einem
zweiten Tenaculum fassen. Perforationstest wiederholen.
3. Uterusperforation: Wenn Verdacht auf eine Perforation besteht,
sollte das Verfahren unverzüglich abgebrochen werden.
Hinweis: Bei einer stark erweiterten Zervix kann am externen
Muttermund CO2 austreten. Unter diesen Bedingungen kann
das CO2-Leck von sichtbaren Bläschen oder einem zischenden
Geräusch begleitet sein.
Hinweis: Beim Befolgen der Schritte zur Fehlerbehebung beim HF-
Controller, Modell 10 für weitere Informationen auf die Schaltfläche
„?“ auf dem Bildschirm drücken und die Scroll-Tasten auf der
rechten Seite verwenden. Um von den zusätzlichen Tipps zur
Fehlerbehebung wieder zum Hauptbildschirm zu gelangen, auf das
„X“ in der rechten oberen Bildschirmecke drücken.
Wenn der Perforationstest nach einer angemessenen Anzahl von
Versuchen der Fehlerbehebung (Schritt 2.36) immer noch fehlschlägt,
muss das Verfahren abgebrochen werden.
VAKUUMALARM
Der Vakuumalarm wird ausgelöst, wenn sich die Vakuumstufe außerhalb
des festgelegten Bereichs befindet. Dies kann als Resultat einer oder
mehrerer der folgenden Konditionen auftreten:
• eine zu stark erweiterte Zervix;
• ein schlechter Kontakt zwischen der Zervixmanschette und dem
äußeren Muttermund;
• das Vakuumsicherheitsventil befindet sich in der geschlossenen
Position;
• eine Blockierung im Filter (oder in beiden Filtern) des Einmalinstruments
oder Trockenmittelfilter; oder
• eine Blockierung innerhalb des Einmalinstruments.
Wenn die Vakuumprüfung fehlschlägt, wird der Bildschirm „Vakuumfehler“
mit einer Kurzfassung der folgenden Tipps zur Fehlerbehebung angezeigt:
• Mit einem 2–3,5 mm Uterusdilatator oder einer Sonde innerhalb des
Vakuumsicherheitsventils behutsam Druck ausüben.
• Die Position der Zervixmanschette überprüfen und sie ggf. neu
positionieren. Die Zervixmanschette mithilfe der daran befindlichen

19
DEUTSCH
Lasche in Richtung des äußeren Muttermunds vorschieben, um
zu gewährleisten, dass diese eng mit dem äußeren Muttermund
abschließt. Es darf aufgrund einer locker auf der Öffnung zum
Uterushalskanal sitzenden Zervixmanschette kein Luftzug durch
die Zervix entstehen. Bei Lufteintritt durch den Uterushalskanal
die Zervixmanschette und den Schaft des Einmalinstruments neu
positionieren, um das Eindringen der Luft zu verhindern.
• Überprüfen, ob sich der Absaugkanister am Einmalinstrument in einer
vertikalen Position befindet, und dass der Schlauch des Instruments
nicht über das Bein der Patientin gelegt ist.
• Alle Schlauchanschlüsse überprüfen, um zu gewährleisten, dass sie fest
angeschlossen sind. Die Schlauchtüllenanschlüsse am Trockenmittelfilter
überprüfen. Den Filter ersetzen, wenn das Trockenmittel eine rosa Farbe
aufweist. Den festen Sitz des Filters in der Nähe des Anschlusses zum
Einmalinstrument an der Vakuum-Rückführungsleitung überprüfen.
• Den Ablationsversuch wiederholen.
Wenn der Bildschirm „Vakuumfehler“ erneut angezeigt wird:
• das Einmalinstrument vom HF-Controller trennen
• Entfernen Sie das Einweginstrument und ersetzen Sie es durch ein
neues Einweginstrument.
• mit dem neuen Instrument einen weiteren Ablationsversuch
unternehmen.
Hinweis: Beim Befolgen der Schritte zur Fehlerbehebung beim
HF-Controller, Modell 10 für weitere Informationen auf die
Schaltfläche „?“ auf dem Bildschirm drücken und die Scroll-Tasten
auf der rechten Seite verwenden. Um von den zusätzlichen Tipps
zur Fehlerbehebung wieder zum Hauptbildschirm zu gelangen, auf
das „X“ in der rechten oberen Bildschirmecke drücken.
Wenn mit dem neuen Instrument ein Vakuumalarm ausgelöst wird, muss
das Verfahren abgebrochen werden:
Hinweis: Wurde das Einmalinstrument nach Abschluss eines
Perforationstests aus der Uterushöhle entfernt, muss ein weiterer
Perforationstest durchgeführt werden, wenn das Einmalinstrument
wieder eingeführt wird (egal, ob der erste Test erfolgreich war oder
nicht), bevor mit einer Ablation begonnen wird.
CO2-Kanister fast oder völlig leer
Es wird der Bildschirm „CO2 auswechseln“ mit einem Bild der
Rückseite des Controllers angezeigt. Es wird ein Signalton erzeugt,
der 1 Mal pro Sekunde ertönt. Alarmmeldungen, die vor dem Alarm
ausgegeben wurden, behalten während dieses Alarmzustands
wegen der Aufforderung zum Auswechseln des CO2-Kanisters ihren
vorherigen Zustand bei. Der Alarmton lässt sich nicht durch Drücken des
Fußschalters ausschalten.
1. Damit der Alarmton aufhört, den CO2-Kanister auswechseln.
Hinweis: Vor Auswechseln des Kanisters muss das
Einmalinstrument nicht aus der Patientin entfernt werden.
2. Das Verfahren fortsetzen.
POSITION ELEKTRODE-Alarm
Die Warnung „Position Elektrode“ wird angezeigt, wenn die Elektrode
nicht vollständig geöffnet ist. Der Controller kann die Ablation nicht
ausführen, wenn die Warnung „Position Elektrode“ angezeigt wird. Wenn
der POSITION ELEKTRODE-Alarm ausgelöst wird, wird der Bildschirm
„Goldnetzelektrode überprüfen“ mit einer Kurzfassung der folgenden
Tipps zur Fehlerbehebung angezeigt:
1. Das proximale Ende des Einmalinstruments behutsam bewegen
und dabei beobachten, ob die Warnung „Position Elektrode“ nicht
mehr angezeigt wird. Wird sie weiterhin angezeigt, folgendermaßen
vorgehen:
2. Behutsam versuchen, das NovaSure-Einmalinstrument neu zu
positionieren:
A. Die Elektrode durch Loslassen des Entriegelungsknopfs am Griff
des Einmalinstruments teilweise in die Hülse zurückziehen;
B Das Einmalinstrument leicht vom Fundus wegziehen;
C. Die Elektrode des Einmalinstruments langsam erneut entfalten
und dabei das Einmalinstrument behutsam hin- und herbewegen
und die Griffe des Einmalinstruments verriegeln; und
D. Erneut unter Befolgung des in Abschnitt 2.26 bis 2.33
beschriebenen Einsetzverfahrens für einen korrekten Sitz des
Einmalinstruments am Fundus sorgen.
3. Bei einem retrovertierten Uterus ist mit besonderer Sorgfalt
vorzugehen, um eine Perforation zu vermeiden. Während des
Einsetzverfahrens mit dem Tenaculum die Zervix behutsam nach
kaudal ziehen und den Griff des Einmalinstruments nach oben in
Richtung Decke anheben (in einer Linie mit der Uterusachse).
4. Wird die Warnung „Position Elektrode“ weiterhin angezeigt, die
Elektrode des Einmalinstruments vollständig zurückziehen und das
Einmalinstrument aus der Patientin entfernen.
5. Das Einmalinstrument außerhalb des Körpers der Patientin entfalten.
Die Goldnetzelektrode darf nicht beschädigt sein und die Warnung
„Position Elektrode“ darf nicht mehr angezeigt werden.
6. Erneut versuchen, das Einmalinstrument nach dem in Abschnitt
2.0 beschriebenen Einsetzverfahren einzuführen, zuentfalten und
korrekt zu positionieren.
7. Wird die Warnung „Position Elektrode“ weiterhin angezeigt, das
Instrument gegen ein neues Einmalinstrument auswechseln.
8. Wird die Warnung „Position Elektrode“ bei einem neuen
Einmalinstrument ebenfalls angezeigt, das Verfahren abbrechen.
Hinweis: Beim Befolgen der Schritte zur Fehlerbehebung beim HF-
Controller, Modell 10 für weitere Informationen auf die Schaltfläche
„?“ auf dem Bildschirm drücken und die Scroll-Tasten auf der
rechten Seite verwenden. Um von den zusätzlichen Tipps zur
Fehlerbehebung wieder zum Hauptbildschirm zu gelangen, auf das
„X“ in der rechten oberen Bildschirmecke drücken.
Bitte lesen Sie die Bedienungsanleitung
auf der nächste Seite weiter. Zusätzliche
Fehlerbehebung.

20
DEUTSCH
Vermutete Uterusperforation
Vor Anwendung von Energie: Während oder nach Anwendung
von Energie:
1. Verfahren abbrechen 1. Verfahren abbrechen
2. Stabilität der Patientin
gewährleisten 2. Stabilität der Patientin
gewährleisten
3. Abklären, ob eine Perforation
vorliegt 3. Bauchverletzung ausschließen
4. Sofern angemessen, neuen
Termin für das Verfahren
vereinbaren
4. Sofern angemessen, neuen
Termin für das Verfahren
vereinbaren
Die Goldnetzelektrode entfaltet sich nicht vollständig und
verriegelt sich nicht im Uterus
1. Die Elektrode teilweise in die Hülse zurückziehen (den vorderen Griff
stationär halten und den hinteren Griff zurück- undvon der Patientin
wegziehen).
2. Das Einmalinstrument in der Uterushöhle neu positionieren.
3. Die Elektrode erneut in der Uterushöhle entfalten.
4. Wenn sich das Einmalinstrument nicht verriegelt, muss es aus dem
Uterus entfernt werden.
5. Das Einmalinstrument auf Schäden prüfen.
6. Versuchen, das Einmalinstrument außerhalb der Patientin zu öffnen
und zu verriegeln.
7. Das Einmalinstrument auswechseln, wenn es beschädigt ist.
8. Ist das Einmalinstrument nicht beschädigt, das Instrument erneut
in die Uterushöhle der Patientin einführen und versuchen, es zu
entfalten.
9. Wenn es nicht möglich ist, das Einmalinstrument auf einen Cornu-zu-
Cornu-Abstand von mindestens 2,5cm zu entfalten, dasVerfahren
abbrechen.
10. Abklären, ob als mögliche Ursache für die fehlgeschlagene Entfaltung
eine Uterusperforation in Frage kommt.
Schwierigkeiten beim Schließen und Entfernen des
Einmalinstruments nach der Ablation
Überprüfen, dass der Entriegelungsknopf gedrückt ist:
• In diesem Fall das Einmalinstrument schrittweise aus der Patientin
entfernen.
• Wenn das nicht der Fall ist, den Entriegelungsknopf drücken und
erneut versuchen, das Einmalinstrument zu schließen. Wenn das
Instrument immer noch schwer zu schließen ist, das Einmalinstrument
schrittweise aus der Patientin entfernen.
Die Anzeige „Eingriff abgeschlossen“ erscheint nicht
auf der HF-Steuereinheit Modell 10, nachdem ein Eingriff
abgeschlossen wurde.
Wenn die Stromversorgung nicht mindestens 30Sekunden angedauert
hat, wird die Anzeige „Eingriff abgeschlossen“ nicht auf der HF-
Steuereinheit Modell 10 angezeigt.
Verfahren nicht abgeschlossen
1. Entfernen Sie das Gerät aus dem Patienten und stellen Sie das Array bereit
a. Vergewissern Sie sich, dass das Array NICHT beschädigt ist
b. Vergewissern Sie sich, dass die Position des Arrays NICHT angezeigt wird
2. Für weitere Hilfe drücken Sie ?
Wenn a und b bestätigt sind, führen Sie das Gerät wieder ein und drücken
Sie den Fußschalter, um die Behandlung erneut zu versuchen.
Wenn ein Problem festgestellt wird, ersetzen Sie das Gerät und starten
Sie den Eingriff neu.
1.Das NovaSure-Einmalinstrument aus dem Uterus nehmen, nachdem
die Elektrode des Einmalinstruments vollständig in die Hülse
zurückgezogen wurde:
A. Den Entriegelungsknopf des Einmalinstruments loslassen.
B. Den vorderen Griff des Einmalinstruments ruhig halten und
C. Den hinteren Griff des Einmalinstruments zurückziehen.
2. Das Einmalinstrument auf Schäden prüfen. Stellen Sie das
Elektrodenarray vollständig außerhalb des Patienten bereit, um zu
sehen, dass die Meldung nicht auf der HF-Steuereinheit Modell 10
angezeigt wird.
3. Wenn das Einweggerät nicht beschädigt ist und die Meldung nicht
auf der HF-Steuereinheit Modell 10 angezeigt wird, erneut einsetzen,
bereitstellen und erneut versuchen.
4. Sollte das Problem weiterhin bestehen, das Instrument gegen ein
neues Einmalinstrument auswechseln.
5. Den Ablationsversuch wiederholen. Sollte das Problem weiterhin
bestehen, das Verfahren abbrechen.
Der Bildschirm „HF AN“ wird nicht auf der HF-Steuereinheit
Modell 10 angezeigt
1. Wenn der NovaSure HF-Controller an eine Stromquelle angeschlossen
und eingeschaltet ist und die Aktivierungstaste (ENABLE) gedrückt
wurde, bei Betätigung des Fußschalters jedoch keine Energie vom
Controller abgegeben wird, die Verbindung des Fußschalters überprüfen.
Außerdem muss der PERFORATIONSTEST abgeschlossen sein.
2. Sollte das Problem weiterhin bestehen, das Verfahren abbrechen.
Beim Drücken der AUFWÄRTS-/ABWÄRTS-Schaltflächen werden
keine Werte angezeigt.
Das Einmalinstrument muss am Controller angeschlossen sein.
DieWerte werden nur dann angezeigt, wenn das Einmalinstrument
ordnungsgemäß an den Controller angeschlossen ist.
Anweisungen zum Auswechseln von Ersatzteilen
Der NovaSure HF-Controller verwendet zwei Sicherungen, die sich in
einem Sicherungshalter im Stromeingangsmodul befinden. Es werden
250-V-Sicherungen vom Typ T5AH verwendet. Zum Zugriff auf das Modul
kann die Klappe des Sicherungshalters mit einem Schlitzschraubenzieher
aufgehebelt werden. Der Sicherungshalter kann dann herausgenommen
werden, um die Sicherungen bei Bedarf auszuwechseln. Nach dem
Einsetzen der Sicherungen sind diese Schritte in umgekehrter Reihenfolge
durchzuführen. Alle möglicherweise defekten NovaSure-Produkte müssen
zur Auswertung an Hologic zurückgesandt werden. Anweisungen zum
Anfordern einer Warenrücknahmeautorisierungsnummer (RMA-Nr.) sind
im Abschnitt „Reparatur-Rücksendungen“ am Ende dieses Handbuchs zu
finden. Das NovaSure-Einmalinstrument nicht wegwerfen.

21
DEUTSCH
Technische Spezifikationen
NovaSure-Einmalinstrument
1. Das NovaSure-Einmalinstrument enthält kein Latex.
2. Das NovaSure-Einmalinstrument ist gemäß FDA-Vorschriften ein
Gerät der Klasse III.
3. Das NovaSure-Einmalinstrument ist gemäß der Verordnung (EU)
2017/742. ein Gerät der Klasse IIB.
4. Der Nenndurchmesser der Spitze des NovaSure-Einmalinstruments
beträgt: 6 mm.
5. Abmessungen des NovaSure-Einmalinstruments: 19” x 6” x 12”
(48.3 cm x 15.2 cm x 5 cm).
6. Das NovaSure-Einmalinstrument hat eine Nennspannung von 153 V.
NovaSure HF-Controller
1. Die NovaSure HF-Steuereinheit kann an Steckdosen mit 100 bis
240 VAC verwendet werden und kann maximal 5 A aufnehmen.
2. Der NovaSure HF-Controller ist gemäß IEC 60601-1 ein
defibrillatorsicheres Gerät der Klasse I vom Typ BF.
3. Der NovaSure HF-Controller ist gemäß FDA-Vorschriften ein Gerät
der Klasse III.
4. Der NovaSure HF-Controller ist gemäß der Verordnung (EU)
2017/742. ein Gerät der Klasse IIB.
5.
Die HF-Steuereinheit wurde getestet und entspricht den Grenzwerten
für Medizinprodukte gemäß IEC 60601-1-2 ED 4.0: 2014.
Diese
Grenzwerte sollen ausreichenden Schutz vor schädlicher Störung in
einer typischen medizinischen Einrichtung gewährleisten. Dieses Gerät
erzeugt und nutzt Hochfrequenzenergie und kann diese abstrahlen.
Wenn es nicht entsprechend den Anweisungen angeschlossen und
verwendet wird, kann dies zu Störungen bei anderen in der Nähe
befindlichen Geräten führen. In Ausnahmefällen können bestimmte
Installationen aber dennoch Störungen verursachen. Sollte dieses Gerät
Störungen bei anderen Instrumenten verursachen, was durch Ein- und
Ausschalten des Geräts bestimmt werden kann, sollte versucht werden,
diese Störungen durch eine oder mehrere der folgenden Maßnahmen
eigenständig zu beheben:
• Ausrichtung oder Standort des Empfängers ändern.
• Den Abstand zwischen den Geräten vergrößern.
• Das Gerät an eine Steckdose anschließen, die einem anderen
Stromkreis als die Steckdose angehört, an die das andere Gerät
bzw. die anderen Geräte angeschlossen ist bzw. sind.
• Den technischen Kundendienst von Hologic (oder den Hersteller des
anderen Geräts) um Hilfe bitten.
6. Der Controller erfüllt die Anforderungen von IEC60601-1/UL60601-1,
IEC60601-2-2 und CSAC22.2Nr.601.1.
7. Der Controller sollte nur in der Originalverpackung von Hologic
versandt werden. Umgebungsanforderungen für Betrieb, Versand und
Lagerung werden nachstehend aufgeführt.
8. Als absolute maximale Spitzenspannung erzeugt der NovaSure
HF-Controller 153Volt. Mit dem HF-Controller verwendetes Zubehör
sollte über eine Nennspannung verfügen, die gleich oder höher als
153 V ist.
9. Als absolute maximale Spitzenleistung erzeugt der NovaSure
HF-Controller 216Watt.
10. NovaSure-RF-Controller-Gewicht: 11 kg, unverpackt.
11. Höhe: 12,5”; Breite: 7,5”; Tiefe: 14,5”
(32 cm x 19 cm x 35.5 cm)..
12. Als maximaler CO2-Druck werden vom NovaSure HF-Controller und
Einmalinstrument 90 ±10mmHg abgegeben. Die maximale CO2-
Flussrate des NovaSure HF-Controllers beträgt bei angeschlossenem
Einmalinstrument 95 ±15ml/min. (Diemaximale CO2-Flussrate des
NovaSure HF-Controllers beträgt ohne angeschlossenes NovaSure-
Einmalinstrument 105 - 130 ml/min.)
13. Der NovaSure-HF-Generator sollte ohne neutrale Elektrode
verwendet werden.
Leistung vs. Widerstand
Gemessene Leistung (Watt)
Lastwiderstand (Ohm)
Tatsächliche Leistung vs. Leistung mit 20 Ohm Lastwiderstand
Tatsächliche Leistung (Watt)
Leistungseinstellwert (Watt)

22
DEUTSCH
Umgebungsbedingungen
NovaSure RF controller
Betriebsbedingungen, unverpackt
Meereshöhe 0 bis 10.000 ft 0 bis 3030 m
Temperatur 10° C bis 40° C 10 °C bis 40 °C
Luftfeuchtigkeit 15 bis 85 % relative Luftfeuchtigkeit
(nichtkondensierend)
Lagerbedingungen, verpackt
Meereshöhe 0 bis 12.120 m
Temperatur –30 °C bis 60 °C
Luftfeuchtigkeit 85 % relative Luftfeuchtigkeit, (nicht
kondensierend)
bis zu 90 % relative Luftfeuchtigkeit, (nicht
kondensierend)
Wichtige Leistungsmerkmale
• Vor dem Einsetzen in den Patienten muss die Luft 10 Sekunden lang
aus dem Gerät abgelassen werden.
• Um den Perforationsdetektortest (Cavity Integrity Assessment,
CIA) zu bestehen, muss für mindestens 3 Sekunden ein Druck von
50 ± 10 mmHg gemessen werden. Andernfalls zeigt der CIA einen
Fehler an. Die HF-Steuereinheit ermöglicht eine Ablation erst, nachdem
der CIA bestanden wurde.
• HF-Leistung: Der Bereich der HF-Leistung liegt zwischen 55 und
180 (+/-20 %) Watt.
• Überwachung des Vakuumdrucks: Während einer Ablation muss
der Vakuumdruck im Bereich von 17,78 ± 5,08 mmHg und
152,4 ± 25,4 mmHg liegen. Wenn der Vakuumdruck diesen Bereich
überschreitet, beendet die Steuereinheit die Ablation.
• Überwachung der Impedanz: Die HF-Steuereinheit beendet die
Ablation, wenn die gemessene Gewebeimpedanz bei ca. 50 Ohm liegt
50 Ohm liegt.
• Zwei-Minuten-Timer: Nach zwei Minuten HF-Energiezufuhr beendet
die Steuereinheit die Ablation.
• Zehn-Minuten-Timeout: Nach Abschluss des Ablationsvorgangs
schaltet sich die Steuereinheit für 10 Minuten aus, wobei die
Steuereinheit während dieser Zeit keine Energie liefern kann.
• DC-Kurzschlussschutz: Erkennt die HF-Steuereinheit einen
Kurzschluss (d. h. <13+/-6 Ohm), wird die Ablation beendet.
Elektromagnetische Sicherheit – Leitlinien
Tabelle 1 - Leitfaden und Erklärung des Herstellers –
elektromagnetische Störfestigkeit
Leitfaden und Erklärung des Herstellers –
elektromagnetische Störfestigkeit
Der NovaSure HF-Controller ist für den Gebrauch in der unten
angegebenen elektromagnetischen Umgebung vorgesehen.
Der Kunde oder Benutzer des NovaSure HF-Controllers sollte
gewährleisten, dass das Instrument nur in einer solchen
Umgebung verwendet wird.
Emissionstest Einhaltung der
Richtlinien Elektromagnetische
Umgebung – Leitlinien
HF-Emissionen
CISPR 11
Gruppe 1 Die NovaSure HF-Steuereinheit
muss elektromagnetische
Energie abstrahlen, um wie
vorgesehen zu funktionieren.
Elektronische Geräte in der
Nähe könnten beeinflusst
werden.
HF-Emissionen
CISPR 11
Klasse A Die NovaSure HF-
Steuereinheit ist für den
Einsatz in professionellen
Gesundheitseinrichtungen
wie Krankenhäusern und
Arztpraxen vorgesehen.
Warnung: Durch ihr
EMISSIONSVERHALTEN
sind diese Geräte ideal
für den Einsatz in
industriellen Bereichen
und Krankenhäusern
geeignet (CISPR 11 Klasse
A). Bei Verwendung in
einer Wohnumgebung
(für die normalerweise
CISPR 11 Klasse B benötigt
wird) bietet das Gerät
möglicherweise keinen
ausreichenden Schutz für
Hochfrequenzkommunika-
tionsdienste. Der Benutzer
muss möglicherweise
Maßnahmen zur
Abschwächung ergreifen
und dafür beispielsweise die
Geräte umstellen oder neu
ausrichten.
Oberschwingungs-
emissionen
IEC 61000-3-2
Klasse A
Spannungs-
schwankungen/
Flickeremis-
sionen IEC 61000-
3-3
Konform
Warnung: Unter bestimmten Umständen besteht die Gefahr von
Verbrennungen an den Kontaktstellen, wenn ein Hochfrequenzgerät
verwendet wird. Der Kontakt von Haut zu Haut sollte vermieden
werden, beispielsweise bei Einführung eines trockenen
Verbandmulls.
Warnung: Beim Einsatz elektrochirurgischer Instrumente können
Lichtbögen entstehen, durch die es zu neuromuskulärer Stimulation

23
DEUTSCH
kommen kann. Wenn dieses Instrument ordnungsgemäß in der
Gebärmutter verwendet wird, ist das Risiko der Muskelstimulation,
besonders des Herzmuskels, gering.
Tabelle 2 -
Leitfaden und Erklärung des Herstellers – elektromagnetische
Emissionen
Leitfaden und Erklärung des Herstellers –
elektromagnetische Emissionen
Der NovaSure HF-Controller ist für den Gebrauch in der unten
angegebenen elektromagnetischen Umgebung vorgesehen.
Der Kunde oder Benutzer des NovaSure HF-Controllers sollte
gewährleisten, dass das Instrument nur in einer solchen Umgebung
verwendet wird.
Störfestig-
keitstest IEC 60601
Prüfpegel Einhaltung
der Richtlinien
Ebene
Elektromagnetische
Umgebung –
Leitfaden
Elektrostatische
Entladung (ESE)
IEC 61000-4-2
±2 kV, ±4 kV,
±8 kV Kontakt ±2 kV, ±4 kV,
±8 kV Kontakt
Das Fußbodenmaterial
sollte Holz, Beton oder
Keramikfliesen sein.
Bei einem syntheti-
schen Fußbodenbelag
sollte die relative
Luftfeuchtigkeit
mindestens 30 %
betragen.
±2 kV, ±4 kV,
±8 kV, ±15 kV
Luft
±2 kV, ±4 kV,
±8 kV, ±15 kV
Luft
Schnelle
transiente
elektrische
Störgröße/Burst
IEC 61000-4-4
±0,5 kV, ±1 kV,
±2 kV für
Stromversor-
gungsleitungen
100 kHz Wieder-
holfrequenz
±0,5 kV, ±1 kV,
±2 kV für
Stromversor-
gungsleitungen
100 kHz Wieder-
holfrequenz
Die Netzspannungs-
qualität sollte einer
typischen Unterneh-
mens- oder Kran-
kenhausumgebung
entsprechen.
Spannungsstoß
IEC 61000-4-5
±0,5 kV, ±1 kV
Leitung(en) zu
Leitung(en)
±0,5 kV, ±1 kV
Leitung(en) zu
Leitung(en)
Die Netzspannungs-
qualität sollte einer
typischen Unterneh-
mens- oder Kran-
kenhausumgebung
entsprechen.
±0,5 kV, ±1 kV,
±2 kV Lei-
tung(en) zu Erde
±0,5 kV, ±1 kV,
±2 kV Lei-
tung(en) zu Erde
Spannungs-
einbrüche,
kurze Unterbre-
chungen und
Spannungs-
schwankungen
der Stromver-
sorgungslei-
tungen
IEC 61000-
4-11
0 % UT;
0,5 Zyklus bei
0°, 45°, 90°,
135°, 180°,
225°, 270°
und 315°
0 % UT;
0,5 Zyklus bei
0°, 45°, 90°,
135°, 180°,
225°, 270°
und 315°
Die Netzspannungs-
qualität sollte
einer typischen
Unternehmens- oder
Krankenhausumgebung
entsprechen. Wenn
das Verfahren mit
dem NovaSure
HF-Controller auch
bei Unterbrechung
der Netzspannung
fortgesetzt werden
muss, wird empfohlen,
den NovaSure
HF-Controller über eine
unterbrechungsfreie
Stromversorgung oder
eine Batterie zu be-
treiben.
0 % UT;
1 Zyklus und
70 % UT;
25/30 Zyklen
Einphasig: bei 0°
0 % UT;
1 Zyklus und
70 %UT;
25/30 Zyklen
Einphasig: bei 0°
0 % UT;
250 Zyklen 0 % UT;
250 Zyklen
Bei diesem
Zustand schaltet
die HF-Steuer-
einheit ab
und kehrt
dann in den
Standby-Modus
zurück.
Abgestrahlte HF
IEC 61000-4-3
3 V/m
80 MHz bis
2,7 GHz
80 % MW bei
1 kHz
3 V/m
80 MHz bis
2,7 GHz
80 % MW bei
1 kHz
Netzfrequenz
50/60Hz
Magnetfeld
IEC 61000-4-8
30 A/m
50 Hz
30 A/m
50 Hz
Die Magnetfelder mit
energietechnischer
Frequenz sollten
einer typischen
Unternehmens- oder
Krankenhausumgebung
entspreche
Hinweis : UT ist die Wechselstrom-Netzspannung vor dem Einsatz des Testniveaus.

24
DEUTSCH
Tabelle 3 -
Leitfaden und Erklärung des Herstellers –
elektromagnetische Emissionen
Leitfaden und Erklärung des Herstellers –
elektromagnetische Emissionen
Der NovaSure HF-Controller ist für den Gebrauch in der unten
angegebenen elektromagnetischen Umgebung vorgesehen. Der Kunde
oder Benutzer des NovaSure HF-Controllers sollte gewährleisten, dass
das Instrument nur in einer solchen Umgebung verwendet wird.
Störfestig-
keitstest IEC 60601
Prüfpege Einhaltung
der Richtlinien
Ebene
Elektromagnetische Um-
gebung –
Leitfaden
Leitungsge-
führte HF
IEC 61000-4-6
3 V
0,15 MHz –
80 MHz
6 V in ISM- und
Amateurfunkbän-
dern zwischen
0,15 MHz und
80 MHz
80 % MW bei
1 kHz
3 V
0,15 MHz –
80 MHz
6 V in ISM- und
Amateurfunk-
bändern zwi-
schen
0,15 MHz und
80 MHz
80 % MW bei
1 kHz
Empfohlener
Mindestabstand
Tragbare HF-
Kommunikationsgeräte
(einschließlich
Perpheralgeräte wie
Antennenkabel und
externe Antennen) sollten
nicht näher als 30cm
(12Zoll) am NovaSure
impedanzgesteuerten
Endometrium-
Ablationssystem,
einschließlich der von
Hologic Inc. spezifizierten
Kabel, verwendet werden.
Andernfalls könnte es zu
einer Verschlechterung
der Leistung dieses
Geräts kommen.
Die Feldstärken
stationärer
Hochfrequenzsender, die
bei der
elektromagnetischen
Untersuchung des
Standorts ermittelt
wurden,
a
sollten für jeden
Frequenzbereich unter dem
Grenzwert liegen.
b
Störungen können in der
Nähe von Geräten auftreten,
die mit dem folgenden
Symbol gekennzeichnet
sind:
Abgestrahlte HF
IEC 61000-4-3
3 V/m
80 MHz bis
2,7 GHz
80 % MW bei
1 kHz
3 V/m
80 MHz bis
2,7 GHz
80 % MW bei
1 kHz
HINWEIS 1: Bei 80 MHz und 800 MHz gilt der höhere Frequenzbereich.
HINWEIS 2: Diese Richtlinien gelten möglicherweise nicht in allen
Situationen. Die Ausbreitung elektromagnetischer Strahlung wird durch die
Absorption und die Reflektion von Strukturen, Gegenständen und Personen
beeinflusst.
a
Die Feldstärken stationärer Sender, wie z. B. Basisstationen für Funktelefone (Handys/Schnurlostelefone)
sowie Sendern für Landfunk, Amateurfunk, UKW/MW-Radio- und Fernsehübertragung können theoretisch
nicht genau vorhergesagt werden. Um die durch stationäre Hochfrequenzsender bedingte elektromagnetische
Umgebung zu beurteilen, sollte eine elektromagnetische Untersuchung des Aufstellungsorts in Betracht gezogen
werden. Wenn die gemessene Feldstärke am Einsatzort des HF-Erzeugers die entsprechenden Grenzwerte
für Hochfrequenzstörungen übersteigt, sollte beobachtet werden, ob der HF-Erzeuger normal arbeitet. Werden
Betriebsstörungen festgestellt, sind weitere Maßnahmen erforderlich, wie z.B. die Ausrichtung oder den Standort
des HF-Erzeugers zu ändern.
b
Im Frequenzbereich 150 kHz bis 80 MHz sollte die Feldstärke unter 3 V/m liegen.
Tabelle 4 - Empfohlene Mindestabstände zwischen tragbaren
und mobilen HF-Kommunikationsgeräten und dem NovaSure
HF-Controller
Tragbare HF-Kommunikationsgeräte (einschließlich Perpheralgeräte
wie Antennenkabel und externe Antennen) sollten nicht näher als
30cm (12Zoll) am NovaSure impedanzgesteuerten Endometrium-
Ablationssystem, einschließlich der von Hologic Inc. spezifizierten Kabel,
verwendet werden. Andernfalls könnte es zu einer Verschlechterung der
Leistung dieses Geräts kommen.
Reinigung und Desinfektion
Für Reinigung und Desinfektion wird die Verwendung nicht entflammbarer
Wirkstoffe empfohlen. Für Reinigung oder Desinfektion verwendete
entflammbare Wirkstoffe oder Lösungsmittel zunächst verdunsten lassen,
bevor das NovaSure-System in Betrieb genommen wird.
Der NovaSure HF-Controller ist unsteril. Zur Reinigung sollten nur die
Oberflächen mit einer milden Reinigungslösung und Wasser abgewischt
werden. Das Gerät nicht in Flüssigkeit eintauchen und keine Flüssigkeit
in die Lüftungsschlitze oder HF-Kabelbereiche eindringen lassen.
Das NovaSure-Einmalinstrument ist ein steriles Einmalinstrument, das
zur Verwendung bei nur einer Patientin bestimmt ist.
• Nicht verwenden, wenn die Verpackung geöffnet oder beschädigt ist.
• Das Einmalinstrument darf nicht wiederverwendet oder resterilisiert
werden.
Keine der Komponenten des NovaSure impedanzgesteuerten
Endometrium-Ablationssystems sterilisieren.

25
DEUTSCH
Teileliste
Bestellinformationen und zugehörige Teile und Zubehör
Produktnummer Beschreibung
RFC2010 NovaSure HF-Controller, Modell 10
814002 Netzkabel, 115 Volt, Nordamerika
814003 Netzkabel, 230 Volt, Europa
814004 Netzkabel, 220 Volt, Großbritannien/Irland
814005 Netzkabel, Dänemark
814009 Netzkabel, Italien
814011 Netzkabel, Schweiz
814015 Netzkabel, Japan
814016 Netzkabel, Österreich
52124-001 Fußschalter
815012 CO2 (USP), Zylinder 5 Stück
NS2013 Kit mit NovaSure-Einmalinstrument für die
impedanzgesteuerte Endometriumablation
300001 Kit zum Versand biogefährlicher Materialien
Entsorgung
Achtung: Das Einmalinstrument muss als biogefährlicher Abfall
behandelt werden und entsprechend den Standardverfahren des
Krankenhauses oder der Praxis entsorgt werden.
Hologic und dessen Vertriebshändler und Kunden in der Europäischen
Gemeinschaft müssen die WEEE-Richtlinie über Elektro- und
Elektronik-Altgeräte (2002/96/EG) einhalten. Hologic engagiert sich
für die Erfüllung der landesspezifischen Anforderungen in Bezug auf
den umweltfreundlichen Umgang mit seinen Produkten. Hologics Ziel
besteht in der Reduzierung des aus der Entsorgung seiner elektrischen
und elektronischen Geräte resultierenden Abfalls. Hologic hält es im
Hinblick auf eine Reduzierung der Menge an Schadstoffen, die in die
Umwelt gelangen, für nützlich, die Elektro- und Elektronik-Altgeräte einer
potenziellen Wiederverwendung, Aufbereitung, einem Recycling oder einer
Rückgewinnung zuzuführen. Die Kunden von Hologic in der Europäischen
Gemeinschaft sind dafür verantwortlich, dass medizinische Geräte, die mit
dem folgenden Symbol gekennzeichnet sind, das darauf hinweist, dass
die WEEE-Richtlinie anzuwenden ist, ohne Genehmigung der örtlichen
Behörden nicht über das Stadtmüllentsorgungssystem entsorgt werden.
Setzen Sie sich zwecks geeigneter Entsorgung des HF-Controllers
in Übereinstimmung mit der WEEE-Richtlinie mit dem technischen
Kundendienst von Hologic in Verbindung.
Garantie
Falls in der Vereinbarung nicht ausdrücklich anders aufgeführt,
gilt Folgendes: i) Für von Hologic hergestellte Geräte wird dem
ursprünglichen Kunden ein (1) Jahr ab Versanddatum, oder falls eine
Installation notwendig ist, ab Installationsdatum („Garantiezeitraum“)
gewährleistet, dass sie im Wesentlichen gemäß den veröffentlichten
Produktspezifikationen funktionieren. ii) Die Gewährleistung für
Röntgenröhren für digitale Mammographie-Aufnahmen gilt für
vierundzwanzig (24) Monate. In diesem Zeitraum gilt die Gewährleistung
für die Röntgenröhren während der ersten zwölf (12) Monate in
vollem Umfang und während der Monate 13–24 auf einer linearen
anteiligen Basis. iii) Für Ersatzteile und aufgearbeitete Teile gilt eine
Gewährleistung für den Rest des Garantiezeitraums bzw. neunzig
(90) Tage ab Versanddatum, je nachdem, welcher Zeitraum länger ist.
iv) Für Verbrauchsmaterialien wird für einen Zeitraum, der mit dem
auf der Packung angegebenen Verfallsdatum endet, gewährleistet,
dass sie gemäß den veröffentlichten Spezifikationen funktionieren.
v) Für lizenzierte Software wird gewährleistet, dass sie gemäß den
veröffentlichten Spezifikationen funktioniert. vi) Für Dienstleistungen wird
die fachgerechte Durchführung gewährleistet. vii) Die Gewährleistung
für nicht von Hologic stammende Geräte wird von ihren jeweiligen
Herstellern angeboten und solche Herstellergarantien erstrecken sich
auf die Kunden von Hologic, soweit vom Hersteller solcher nicht von
Hologic stammenden Geräte genehmigt. Hologic gewährleistet nicht
die ununterbrochene oder fehlerfreie Verwendung von Produkten oder
die Verwendbarkeit seiner Produkte mit nicht von Hologic stammenden
autorisierten Produkten Dritter.
Diese Garantien gelten nicht für Artikel, die: (a) von anderem als von
Hologic autorisiertem Personal repariert, bewegt oder geändert wurden;
(b) physischer (einschließlich thermischer und elektrischer) Belastung,
Zweckentfremdung oder unsachgemäßem Gebrauch ausgesetzt wurden;
(c) auf jegliche Weise aufbewahrt, gewartet oder bedient wurden, die
nicht den anwendbaren Spezifikationen oder Anweisungen von Hologic
entspricht, was auch die Verweigerung des Kunden einschließt, von
Hologic empfohlene Software-Aktualisierungen vorzunehmen; oder
(d) als gelieferte Ware ausgewiesen wird, die nicht einer Garantie von
Hologic unterliegt, bzw. die als Vorveröffentlichung oder „wie besehen“
verkauft wird.
Technischer Kundendienst und Informationen zur
Warenrücknahme
Warnung: Durch Fallenlassen des HF-Controllers wird die Garantie
ungültig und der Controller kann so stark beschädigt werden, dass
keine Reparatur mehr möglich ist. Wir raten sehr zu einem stabilen
Wagen, auf dem der Controller festgeschnallt und stabilisiert wird,
um die Gefahr des Herunterfallens zu reduzieren. Beim Transport
des HF-Controllers zu einer externen Einrichtung ist besondere
Vorsicht geboten. Bei Fragen zum HF-Controller die Nummer
1-800-442-9892 oder (508) 263-2900 anrufen.
Servicemitarbeiter
Sollte der NovaSure HF-Controller funktionsuntauglich werden, sind
vom technischen Kundendienst von Hologic Anweisungen und eine
Warenrücknahmeautorisierungsnummer (RMA-Nr.) erhältlich. Den Controller
reinigen und entsprechend verpacken und für Reparaturzwecke an die
unten aufgeführten autorisierten Kundendienststellen zurücksenden. Ist
der Garantiezeitraum für den Controller abgelaufen, wird bei Annahme und
Prüfung des NovaSure HF-Controllers eine angemessene Handhabungs-
und Reparaturgebühr erhoben.

26
DEUTSCH
Weitere Informationen
Um technische Unterstützung oder Informationen zu Bestellungen zu
erhalten, wenden Sie sich in den USA bitte an:
Hologic, Inc.
250 Campus Drive
Marlborough, MA 01752 USA
Telefon: 800-442-9892
(gebührenfrei in den USA)
www.hologic.com
Hinweis: Alle Vorfälle oder Probleme im Zusammenhang, dass es
sich um ein Sicherheitsproblem handelt, sollten dem technischen
Kundendienst von Hologic mitgeteilt werden.
Internationale Kunden wenden sich bitte an ihren Händler oder
zuständigen Hologic-Vertreter:
Hologic BV
Da Vincilaan 5
1930 Zaventem
Belgium
Tel: +32 2 711 46 80
Fax: +32 2 725 20 87
Richten Sie Beanstandungen oder Probleme mit der Qualität,
Zuverlässigkeit, Sicherheit oder Leistung dieses Produkts an Hologic.
Wenn das Produkt eine Verletzung des Patienten verursacht oder erzeugt
hat, melden Sie den Vorfall unverzüglich dem autorisierten Vertreter
von Hologic und der zuständigen Behörde des jeweiligen Mitgliedstaats
oder Landes. Die zuständigen Behörden für Medizinprodukte sind in der
Regel das Gesundheitsministerium der einzelnen Mitgliedstaaten oder
eine Stelle innerhalb des Gesundheitsministeriums.
Reparatur-Rücksendungen
Vor der Rücksendung gebrauchter oder nicht gebrauchter
Produkte an Hologic, die möglicherweise defekt sind, die folgenden
Anweisungen lesen.
Wenn das NovaSure-Einmalinstrument oder der HF-Controller nicht
bestimmungsgemäß arbeitet, setzen Sie sich mit dem technischen
Kundendienst von Hologic in Verbindung. Wenn das Produkt aus
irgendeinem Grunde an Hologic zurückgesendet wird, gibt der technische
Kundendienst eine Warenrücknahmeautorisierungsnummer (RMA-Nr.) und,
falls zutreffend, ein Kit zum Versand biogefährlicher Materialien aus.
Bei der Rückgabe von HF-Controllern die Anweisungen des technischen
Kundendienstes befolgen. Den HF-Controller vor der Rücksendung
reinigen und gewährleisten, dass dem zurückgesendeten Produkt alle
Zubehörteile beiliegen.
Die Rücksendung benutzter oder geöffneter Einmalinstrumente hat gemäß
den mit dem von Hologic gelieferten Kit zum Versand biogefährlicher
Materialien zur Verfügung gestellten Anweisungen zu erfolgen.
Glossar der Symbole
Symbole Standard-refe-
renz- und Sym-
bolnummer
Bezeichnung
des Symbols Beschreibung des Sym-
bols
EC R
EP
EN ISO 15223-1,
5.1.2
Autorisierte
Vertretung in
der Europäi-
schen Gemein-
schaft
Gibt den Bevollmächtigten
in der Europäischen Ge-
meinschaft an.
IEC 60601-1,
Tabelle D.1, 1
IEC 60417, 5032
Wechselstrom
(AC)
Auf dem Typenschild wird
angegeben, dass das Gerät
nur für Wechselstrom
geeignet ist; um geeignete
Anschlüsse zu finden.
EN ISO 15223-1,
5.3.9
ISO 7000, 2621
Luftdruck-be-
grenzung
Gibt den Bereich des at-
mosphärischen Drucks an,
dem das Medizinprodukt
sicher ausgesetzt werden
kann.
EN ISO 15223-1,
5.1.5
ISO 7000, 2492
Chargennum-
mer
Gibt den Chargencode des
Herstellers an, damit die
Charge oder das Los identi-
fiziert werden kann.
CO2N/A Kohlendioxid Zeigt Kohlendioxid an.
EN ISO 15223-1,
5.1.6
ISO 7000, 2493 Bestellnummer
Gibt die Katalognummer
des Herstellers an, damit
das Medizinprodukt identi-
fiziert werden kann.
N/A
Kategorie
Nicht-AP-Ge-
räte
Identifiziert Geräte der Ka-
tegorie Nicht-AP.
EN ISO 15223-1,
5.4.4
ISO 7000, 0434A
IEC 60601-1,
Tabelle D.1, 10
Achtung
Zeigt an, dass bei der Be-
dienung des Geräts oder
der Steuerung in der Nähe
des Symbols Vorsicht
geboten ist, oder dass
die aktuelle Situation die
Aufmerksamkeit des Be-
dieners oder ein Eingreifen
des Bedieners erfordert,
um unerwünschte Folgen
zu vermeiden.
Europäische
Richtlinie 93/42/
EWG über Me-
dizinprodukte,
Artikel17 und
AnhangXII
Europäische
Verordnung
2017/745 über
Medizin-produk-
te, AnhangV
CE-Zeichen
mit Kennzahl
der benannten
Stelle
Zeigt an, dass das Medizin-
produkt mit der europäi-
schen Richtlinie 93/42/
EWG über Medizinprodukte
übereinstimmt und die
geltenden Gesundheits-,
Sicherheits- und Umwelt-
anforderungen erfüllt. Ist
das Zeichen mit einer
Nummer versehen, wird die
Konformität von der ange-
gebenen benannten Stelle
überprüft.

27
DEUTSCH
Symbole Standard-refe-
renz- und Sym-
bolnummer
Bezeichnung
des Symbols Beschreibung des Sym-
bols
EN ISO 15223-1,
5.4.3
ISO 7000, 1641
IEC 60601-1,
Tabelle D.1, 11
Gebrauchs-
anweisung
beachten
Weist darauf hin, dass der
Benutzer die Bedienungs-
anleitung zurate ziehen
muss.
CC
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 6049
Herstellung-
sland
Zur Identifizierung des
Herstellungslandes der
Produkte.
IEC 60601-1,
Tabelle D.1, 24
IEC 60417, 5036
Gefährliche
Spannung
Hinweis auf Gefahren,
die sich aus gefährlichen
Spannungen ergeben.
EN ISO 15223-1,
5.1.3
ISO 7000, 2497
Herstellungs-
datum Gibt das Herstellungsdatum
des Medizinprodukts an.
IEC 60601-1,
Tabelle D.1, 26
IEC 60417, 5334
Defibrillator-
sicheres Gerät
vom Typ BF
Zur Identifizierung eines
defibrillationssicheren
Anwendungsteils vom Typ
BF, das mit IEC 60601-1
konform ist.
EN ISO 15223-1,
5.2.6
ISO 7000, 2608
Nicht erneut
sterilisieren
Kennzeichnet ein Medizin-
produkt, das nicht resterili-
siert werden darf.
EN ISO 15223-1,
5.4.2
ISO 7000, 1051
IEC 60601-1,
Tabelle D.1, 28
Nicht zur Wie-
der-verwen-
dung
Kennzeichnet ein Medizin-
produkt, das nur zur einmaligen
Verwendung bestimmt ist.
ISO 7000, 2403
ISO 780 Nicht über „n“
hoch stapeln
Hinweis, dass nicht mehr
Artikel als die angegebene
Anzahl übereinander
gestapelt werden dürfen;
entweder wegen der Be-
schaffenheit der Transport-
verpackung oder wegen
der Beschaffenheit der
Teile an sich.
EN ISO 15223-1,
5.2.8
ISO 7000, 2606
Bei beschädig-
ter Verpackung
nicht verwen-
den
Gibt an, dass ein Medizin-
produkt nicht verwendet
werden sollte, wenn die
Verpackung beschädigt
oder geöffnet wurde, und
dass der Benutzer für zu-
sätzliche Informationen
die Bedienungsanleitung
konsultieren sollte.
Symbole Standard-refe-
renz- und Sym-
bolnummer
Bezeichnung
des Symbols Beschreibung des Sym-
bols
IEC 60601-1,
Tabelle D.1, 8
IEC 60417, 5021
Potenzialausg-
leich
Zur Identifizierung der An-
schlüsse, die, wenn sie mi-
teinander verbunden sind,
die verschiedenen Teile
eines Geräts oder eines
Systems auf das gleiche
Potential bringen, wobei es
sich nicht unbedingt um
das Erd-/Masse-Potential
handelt, z.B. für die lokale
Bindung.
WEEE-Richtlinie
2002/96/EC
2012/19/EC
EN 60417, 6414
Europäischen
Richtlinie
2002/96/EG
über Elektro-
und Elektro-
nik-Altgeräte
(WEEE) ent-
sorgt werden.
Weist auf die Notwen-
digkeit der getrennten
Sammlung von Elektro-
und Elektronik-Altgeräten
(WEEE) hin.
ISO 7010
ISO 3864-2,
M002
Gebrauchs-
anleitung
befolgen.
Gibt an, dass die Bedie-
nungsanleitung/Broschüre
gelesen werden muss.
IEC 60417, 5114 Fußschalter
Zur Identifizierung eines
Fußschalters oder die
Verbindung für einen
Fußschalter.
EN ISO 15223-1,
5.3.1
ISO 7000, 0621
ISO 780
Zerbrechlich
Kennzeichnet ein Medizin-
produkt, das bei unvorsi-
chtiger Handhabung kaputt
gehen oder beschädigt
werden kann.
IEC 60143-1,
5016 Sicherung Zur Identifizierung von Si-
cherungskästen oder deren
Position.
HP N/A Hoher Druck Zeigt hohen Druck an.
EN ISO 15223-1,
5.3.8
ISO 7000, 2620
Luftfeuchtig-
keitsbegren-
zung
Gibt den Bereich der Luft-
feuchtigkeit an, dem das
Medizinprodukt sicher aus-
gesetzt werden kann.
EN ISO 15223-1,
5.3.4
ISO 7000, 0626
ISO 780
Vor Nässe
schützen
Kennzeichnet ein Medizin-
produkt, das vor Feuchtig-
keit geschützt werden
muss.
EN ISO 15223-1,
5.3.4
ISO 7000, 0626
ISO 780
Vor Nässe
schützen
Kennzeichnet ein Medizin-
produkt, das vor Feuchtig-
keit geschützt werden
muss.

DEUTSCH
28
AW-22724-801 Rev. 001
04/2022
Symbole Standard-refe-
renz- und Sym-
bolnummer
Bezeichnung
des Symbols Beschreibung des Sym-
bols
EN ISO 15223-1,
5.1.1
ISO 7000, 3082 Hersteller Gibt den Hersteller des
Medizinprodukts an.
ISO/DIS 15223-
1, 5.7.7 Medizin-
produkt
Gibt an, dass es sich bei
dem Artikel um ein Mediz-
inprodukt handelt.
N/A Kein Öl Zeigt an: kein Öl.
EN ISO 15223-1,
5.1.7
ISO 7000, 2609 Unsteril
Kennzeichnet ein Medizin-
produkt, das keinem
Sterilisationsprozess unter-
zogen wurde.
EN ISO 15223-1,
Anhang B Enthält keinen
Naturlatex
Gibt an, dass kein trock-
ener Naturkautschuk
oder Naturkautschuklatex
vorhanden ist.
ISO 7000, 2794 Verpackungs-
einheit Gibt die Anzahl der Teile im
Paket an.
FDA 21 CFR 801 Verschreibung-
spflichtig
Achtung: Laut Bundes-
gesetz (USA) darf dieses
Produkt nur an einen Arzt
oder auf dessen Anordnung
verkauft werden.
IEC 60417, 5140
Nicht ionisie-
rende elektro-
magnet-ische
Strahlung
Zum Hinweis auf allgemein
erhöhte, potenziell gefähr-
liche Werte nicht ionisie-
render Strahlung oder zur
Kennzeichnung von Ge-
räten oder Systemen z.B.
im medizinischen Elektro-
bereich, die HF-Sender
enthalten oder die gezielt
elektromagnet-ische HF-
Energie zur Diagnose oder
Behandlung einsetzen.
EN ISO 15223-1,
5.1.7
ISO 7000, 2498 Seriennummer
Gibt die Seriennummer
des Herstellers an, damit
ein spezifisches Medizin-
produkt identifiziert werden
kann.
ISO/DIS 15223-
1, 5.7.11
ISO 7000, 3707
Steriles
Einweg-Barri-
eresystem
Gibt ein steriles Einweg-
Barrieresystem an.
Symbole Standard-refe-
renz- und Sym-
bolnummer
Bezeichnung
des Symbols Beschreibung des Sym-
bols
EN ISO 15223-1,
5.2.3
ISO 7000, 2501
Sterilisation
mit Ethylenoxid
Kennzeichnet ein Medizin-
produkt, das mit Ethylen-
oxid sterilisiert wurde.
EN ISO 15223-1,
5.3.7
ISO 7000, 0632
Temperatur-
grenze
Gibt die Temperaturgrenzen
an, innerhalb derer das
Medizinprodukt sicher be-
trieben werden kann.
ISO 7000, 0623
ISO 780, 0623
IATA 2004
Diese Seite
oben
Zeigt die korrekte aufrechte
Position der Transportver-
packung an.
UDI
ISO/DIS 15223-
1, 5.7.10
Eindeutige
Geräteidentifi-
zierungsnum-
mer
Gibt Geräteidentifizier-
ungsnummern und Produk-
tidentifizierungsnummern
des Medizinprodukts an.
EN ISO 15223-1,
5.1.4
ISO 7000, 2607 Verfallsdatum
Gibt das Datum an, nach
dem das Medizinprodukt
nicht mehr verwendet wer-
den darf.
Hologic, NovaSure und dazugehörige Logos sind Marken bzw.
eingetragene Marken von Hologic Inc. bzw. ihren Tochtergesellschaften
in den USA und/oder anderen Ländern.
Das NovaSure impedanzgesteuerte Endometrium-Ablationssystem
wirdvon Hologic Inc. hergestellt und vertrieben.
©2014-2022 Hologic Inc.

1
ITALIANO
NovaSure®
Istruzioni per l’uso e manuale operativo
del controller
Sommario
Lista di controllo per il medico .........................1
Descrizione del sistema ..............................1
Indicazioni .........................................3
Gruppo di pazienti target. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Benefici clinici previsti per le pazienti ...................3
Utente previsto ......................................3
Controindicazioni ....................................3
Avvertenze .........................................4
Precauzioni ........................................5
Dati clinici NovaSure a 3 anni ..........................6
Effetti collaterali ...................................6
Possibili complicanze postoperatorie ....................6
Altri effetti collaterali ................................6
Studio clinico ......................................7
Selezione delle pazienti. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Consulenza alle pazienti ............................10
Preparazione della paziente all’intervento ............... 10
Sistema di ablazione endometriale NovaSure a impedenza
Istruzioni per l’uso ....................................10
Funzionamento del controller RF modello 10 ............16
Manutenzione periodica e assistenza ..................17
Icone dello schermo del controller RF NovaSure modello 10 17
Risoluzione delle condizioni di allarme più comuni ........18
Allarme del vuoto .. ...............................18
Istruzioni per la sostituzione di componenti .............20
Specifiche tecniche .................................21
Dispositivo monouso NovaSure ....................... 21
Controller RF NovaSure .............................21
Condizioni ambientali ..............................22
Caratteristiche importantisul funzionamento: ............22
Informazioni sulla sicurezza elettromagnetica ............22
Pulizia e disinfezione ..............................24
Lista delle parti ................................... 25
Smaltimento .......................................25
Garanzia .......................................... 25
Assistenza tecnica e informazioni per la restituzione
dei prodotti. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Glossario dei simboli ...............................26
ATTENZIONE: LA LEGGE FEDERALE STATUNITENSE LIMITA
LA VENDITA DI QUESTO DISPOSITIVO AI MEDICI DOTATI DI
ADEGUATA PREPARAZIONE O SU PRESCRIZIONE DEGLI STESSI.
Leggere tutte le istruzioni, precauzioni e avvertenze prima dell’uso.
Il mancato rispetto delle istruzioni o degli avvisi e precauzioni può
causare serie lesioni alla paziente.
Nota: il manuale fornito in dotazione con il dispositivo monouso
potrebbe contenere una versione delle istruzioni relative al sistema
NovaSurepiù recente rispetto al manuale fornito con il controller.
Il dispositivo monouso NovaSurenon deve essere usato con altri
controller o generatori di radiofrequenza, così come il controller RF
NovaSurenon deve essere utilizzato con altri dispositivi monouso.
Il dispositivo monouso NovaSure non contiene lattice.
Lista di controllo per il medico
Il medico deve:
• avere esperienza con le procedure relative alla cavità uterina (quali, ad
esempio, l’inserimento di spirali, dilatazione e raschiamento), nonché
una formazione e una conoscenza adeguate del sistema NovaSure;
• rivedere le istruzioni e familiarizzare con esse e assicurarsi di ricevere
un training adeguato tramite la NovaSure o altro medico autorizzato;
• assicurarsi di conoscere la sequenza esatta delle operazioni da
eseguire, secondo quanto riportato nelle istruzioni per l’uso e nella
sezione relativa alla risoluzione dei problemi del presente manuale,
onde poter interrompere, risolvere o continuare il trattamento nel
caso in cui il sistema rileva una perdita di CO2 nel corso dell’esame
condotto per valutare l’integrità della cavità. La presenza di una
perdita indica una possibile perforazione dell’utero.
Anche il personale ausiliario deve familiarizzare con il materiale
di formazione prima di usare il sistema NovaSure e conoscerne le
istruzionid’uso.
Descrizione del sistema
Il sistema di ablazione endometriale NovaSure a impedenza consiste di:
un dispositivo monouso NovaSure con relativo cavo di collegamento, un
controller RF NovaSure, il contenitore NovaSure per CO2, il disidratante,
l’interruttore a pedale e il cavo di alimentazione. I diversi componenti
sono progettati per funzionare insieme come un unico sistema.
Dispositivo monouso NovaSure con cavo di collegamento,
incluso il disidratante della linea di suzione

2
ITALIANO
Descrizione del dispositivo monouso NovaSure
Il dispositivo monouso NovaSure è composto da un array di elettrodi
bipolari modellabili per l’uso su una singola paziente, montato su una
struttura espandibile in grado di creare una lesione confluente sull’intera
superficie interna della cavità uterina. Tale dispositivo viene inserito nella
cavità uterina per via transcervicale. Dopo l’inserimento transcervicale
nella cavità uterina, la guaina viene retratta per consentire il dispiegamento
dell’array di elettrodi bipolari e il suo adeguamento alla cavità uterina.
L’array di elettrodi bipolari è formato da tessuto poroso metallizzato che
consente il passaggio continuo del vapore e dell’umidità rimossi dal
tessuto dissiccato. Il dispositivo monouso funziona unitamente all’apposito
controller RF NovaSure per consentire la rimozione totale e personalizzata
dell’endometrio in circa 90secondi, senza dover ricorrere a isteroscopia
o trattamento preliminare dell’endometrio. La particolare configurazione
dell’array di elettrodi e la potenza predeterminata del controller consentono
un controllo totale della profondità di ablazione nell’utero, che viene
mantenuta uguale o minore di 10 cm, con una distanza minima tra corni di
2,5cm.
Nel corso della procedura di ablazione il flusso di energia in radiofrequenza
vaporizza e coagula l’endometrio, indipendentemente dal suo spessore, e
disidrata e quindi coagula la superficie del miometrio sottostante.
Il controller calcola automaticamente il livello di potenza ottimale in
Watt necessario per il trattamento della cavità uterina, sulla base delle
dimensioni dell’utero. Man mano che la profondità del tessuto distrutto
si avvicina alla profondità ottimale, l’impedenza del tessuto aumenta
causando la disattivazione automatica dell’erogazione di potenza da
parte del controller. Si tratta pertanto di una procedura autoregolata. Il
sangue, la soluzione salina ed eventuali altri liquidi presenti nella cavità
uterina durante la procedura, così come il vapore rilasciato dal tessuto
dissiccato, vengono rimossi per mezzo di suzione continua e automatica.
Il dispositivo monouso viene collegato al controller per mezzo di un cavo
contenente il cavo RF, di tubi di suzione (utilizzati per il monitoraggio della
pressione durante l’esame di valutazione dell’integrità della cavità e per la
suzione durante il ciclo di ablazione) e di un tubo di ritorno del vuoto (usato
per l’erogazione di CO2 durante l’esame e per il monitoraggio del vuoto
durante l’ablazione).
Il dispositivo monouso è stato sterilizzato con ossido di etilene (EO).
Controller RF NovaSure
modello 10
Descrizione del controller RF NovaSure
Il controller RF NovaSure è un generatore di potenza costante con una
capacità di erogazione massima pari a 180 watt. Il controller calcola
automaticamente la potenza in uscita sulla base della lunghezza
(misurazione dell’isterometria meno la lunghezza del canale endocervicale)
e della larghezza della cavità uterina, secondo i dati immessi nel controller
dall’operatore. Il controllo dell’impedenza del tessuto durante l’ablazione
regola automaticamente la profondità di ablazione endo e miometriale. La
procedura NovaSure termina automaticamente quando la vaporizzazione
dell’endometrio e la disseccazione della superficie del miometrio
raggiungono un’impedenza di circa 50 ohm nel punto di interfaccia tra il
tessuto e l’elettrodo o quando la durata totale del trattamento raggiunge
i due minuti. L’esame di valutazione dell’integrità della cavità è parte
integrante del controller. Esso serve per determinare se vi siano difetti o
perforazioni della parete uterina. Una volta che il dispositivo monouso è
posizionato nella cavità uterina, viene erogata CO2 alla cavità, attraverso
il lume centrale del dispositivo e il tubo del vuoto, a una pressione e a
un flusso sicuri. Se la pressione della CO2 all’interno della cavità uterina
rimane invariata per un breve periodo di tempo, il sistema di valutazione
dell’integrità della cavità consente di attivare il controller RF NovaSure e di
procedere con il trattamento. Una pompa del vuoto contenuta all’interno
del controller RF NovaSure crea e mantiene il vuoto nella cavità uterina
per la durata della procedura di ablazione. Una volta stabilizzato il vuoto, il
livello del vuoto è controllato durante la restante parte della procedura.

3
ITALIANO
Descrizione del disidratante della
linea di suzione NovaSure
Il disidratante della linea di suzione
NovaSure è un componente sterile, da
usarsi su una singola paziente, che viene
collegato in linea con il tubo di suzione
prima di collegare il dispositivo monouso
con il controller RF NovaSure. Durante
la procedura di ablazione, il disidratante
assorbe l’umidità rimossa dalla cavità
uterina tramite il tubo di suzione.
Descrizione dell’interruttore a
pedale NovaSure
L’interruttore a pedale NovaSure è un
interruttore pneumatico collegato al
pannello anteriore del controller RF
NovaSure. Viene usato per attivare il
controller NovaSure RF e non contiene
componenti elettriche.
Lorem ipsum
Descrizione del contenitore per CO2
NovaSure
Il contenitore di CO2 NovaSure è un
contenitore da 16 grammi (standard
USP) per CO2. Esso viene collegato a un
regolatore posto sul pannello posteriore
del controller RF NovaSure prima che
venga attivato il controller RF NovaSure.
La CO2 viene usata dal sistema di
valutazione dell’integrità della cavità per
pressurizzare la cavità uterina.
Il contenitore di CO2 cod. art. 815012
contiene CO2 al 99%.
Descrizione del cavo di
alimentazione c.a. NovaSure
Il cavo di alimentazione del sistema
NovaSure è un cavo di categoria
ospedaliera che collega il controller RF
NovaSure all’alimentazione. La presa
per il cavo di alimentazione (modulo di
ingresso dell’alimentazione) è posta sul
pannello posteriore del controller.
Indicazioni
Il sistema NovaSure viene utilizzato per l’ablazione dell’endometrio
nelle donne in premenopausa soggette a menorragia (sanguinamento
eccessivo) di origine benigna e che non intendano più avere gravidanze.
Gruppo di pazienti target
Il sistema NovaSure è indicato per l’uso su donne in premenopausa
soggette a menorragia (sanguinamento eccessivo) di origine benigna che
non intendono più avere gravidanze.
Benefici clinici previsti per le pazienti
Ridurre o eliminare il sanguinamento nelle donne in premenopausa con
mestruazioni abbondanti di origine benigna che non intendono più avere
gravidanze
Utente previsto
Il sistema NovaSure deve essere utilizzato sotto la supervisione e la
guida di un ostetrico-ginecologo oppure di un ginecologo o chirurgo
ginecologo. Il medico si occuperà fondamentalmente di utilizzare
il dispositivo NovaSure e potrà fornire istruzioni all’assistente sul
funzionamento del controller RF e attivare quest’ultimo mediante
l’interruttore a pedale. Il controller RF sarà azionato da un sistema
assistente non sterile.
Il medico deve:
• Avere sufficiente esperienza nell’esecuzione di procedure all’interno
della cavità uterina come l’inserimento di IUD o la dilatazione e il
curettage (D&C) e disporre di un’adeguata formazione, conoscenza
e familiarità con l’uso del sistema NovaSure.
• Riesaminare e avere la piena conoscenza delle istruzioni nonché
completare la formazione NovaSure o essere addestrato da un
medico qualificato.
Prima di utilizzare il sistema NovaSure, il personale coadiuvante deve
avere familiarità con le Istruzioni per l’uso e gli altri materiali formativi.
Contraindicazioni
Il sistema di ablazione endometriale NovaSure a impedenza è
controindicato nei seguenti casi:
• pazienti in gravidanza o che prevedono una gravidanza per il futuro;
legravidanze che hanno luogo dopo un’ablazione possono essere
rischiose per la madre e per il feto;
• pazienti con carcinoma accertato o sospetto dell’endometrio (tumore
dell’utero) o condizioni maligne dell’endometrio, quali iperplasie
adenomatose non risolte;
• pazienti con condizioni anatomiche (ad esempio, cesarei tradizionali
precedenti o miomectomia transmurale) o patologiche (ad esempio,
terapia medica a lungo termine) suscettibili di indebolire il miometrio;
• pazienti con infezione attiva dei genitali o del tratto urinario al
momento della procedura (ad esempio, cervicite, vaginite, endometrite,
salpingite o cistite);
• pazienti con spirale contraccettiva (IUD) inserita; la presenza della
spirale nella cavità uterina può interferire con la procedura NovaSure;
• pazienti con una cavità uterina di lunghezza inferiore a 4 cm; la
lunghezza minima dell’array di elettrodi è di 4 cm; il trattamento
di unacavità uterina di lunghezza inferiore a 4 cm causerà lesioni
termiche al canale endocervicale;
• pazienti con una cavità uterina di larghezza inferiore a 2,5 cm,
secondo quanto determinato dall’apposito selettore WIDTH
(LARGHEZZA) del dispositivo monouso, una volta che quest’ultimo
èstato posizionato edispiegato;
• pazienti con malattia infiammatoria pelvica attiva.

4
ITALIANO
Avvertenze
Il mancato rispetto delle istruzioni o degli avvisi e precauzioni
può causare serie lesioni alla paziente.
Il dispositivo monouso NovaSure deve essere utilizzato
esclusivamente con il controller RF NovaSure.
La procedura NovaSure è concepita per essere eseguita una
sola volta e con un unico intervento. L’esecuzione di molteplici
cicli terapeutici con il sistema NovaSure nel corso di un unico
intervento può causare lesioni termiche all’intestino.
Perforazione dell’utero
• Prestare attenzione a non perforare la parete uterina durante la
misurazione, la dilatazione o l’inserimento del dispositivo monouso.
• Se l’inserimento del dispositivo monouso nel canale cervicale risulta
difficile, determinare sulla base della propria esperienza se sia
necessario dilatare ulteriormente.
• Prima del trattamento, il sistema NovaSure esegue un esame per
controllare l’integrità della cavità uterina ed emette un segnale
acustico nel caso di condizioni indicanti la presenza di una
perforazione (punto 2.36). (Nonostante l’esame sia progettato
per identificare una perforazione della parete uterina, si tratta
solamente di un esame indicativo, non in grado di rilevare tutte
le perforazioni possibili in una varietà di condizioni. Spetta al
medico emettere un giudizio clinico sulla base della propria
esperienza).
• Se si sospetta una perforazione dell’utero, terminare
immediatamente la procedura.
• Se, dopo vari tentativi, l’esame di valutazione dell’integrità della
cavità non riesce, attenersi a quanto descritto nella sezione
relativa alla risoluzione dei problemi (punto 2.36) e interrompere
la procedura.
• Nel caso di pazienti per le quali si sospetti una perforazione della
parete uterina, eseguire le analisi necessarie a determinare o meno
lapresenza di una perforazione prima della dimissione.
Informazioni generali
• L’ablazione endometriale con il sistema NovaSure non è una procedura
di sterilizzazione. Pertanto, la paziente deve essere consigliata sugli
appropriati metodi anticoncezionali.
• L’ablazione endometriale non elimina la possibilità di iperplasia
endometriale o adenocarcinoma dell’endometrio e può anzi rendere più
difficile per un medico l’individuazione e la diagnosi di tali patologie.
• L’ablazione endometriale deve essere usata esclusivamente sulle donne
che non desiderano avere altre gravidanze, poiché la possibilità di una
gravidanza risulta molto diminuita dopo la procedura. Le gravidanze che
hanno luogo dopo un’ablazione possono essere rischiose per la madre e
per il feto.
• Le pazienti sottopostesi ad ablazione endometriale e che
precedentemente si sono sottoposte a legatura delle tube presentano
un rischio maggiore di sviluppare la sindrome da sterilizzazione delle
tube post-ablazione, condizione che può richiedere un’isterectomia
peressere risolta. Questa condizione può insorgere fino a 10 anni
dopo la procedura.
• Si può presentare un rischio per la paziente laddove le procedure
NovaSure sono eseguite in presenza di un micro-inserto in metallo
conduttivo dal punto di vista termico ed elettrico, nel caso in cui tale
inserto non sia posizionato in modo corretto (ad es. con perforazione
della tuba di Faloppio o del miometrio). In questi casi è possibile che
il calore venga allontanato dall’area di trattamento desiderata verso
altri tessuti e organi a contatto con l’oggetto conduttivo. Questo
potrebbe essere sufficiente a causare ustioni localizzate ed è pertanto
imprescindibile verificare il corretto posizionamento di eventuali
micro-inserti in metallo prima di eseguire la procedura NovaSure.
Informazioni tecniche
• Non usare il dispositivo monouso sterile, se la confezione appare
danneggiata o se presenta segni di manomissione.
• Il dispositivo monouso è da usarsi su una singola paziente. Non riusare
e non risterilizzare il dispositivo monouso. Il rischio del riutilizzo del
dispositivo monouso comprende, senza pretesa di completezza:
• inefficacia dell’intervento
• infezione (di entità importante)
• scossa elettrica
• trasmissione di patologie comunicabili
• lacerazione cervicale
• perforazione dell’utero
• Nel caso in cui, appena prima di eseguire il trattamento NovaSure,
siastata eseguita una procedura isteroscopica con soluzione
ipotonica, irrigare la cavità uterina con soluzione fisiologica prima di
eseguire la procedura NovaSure. La presenza di fluido ipotonico può
ridurre l’efficacia del sistema NovaSure.
• All’inserire il dispositivo monouso nel controller ha inizio il flusso di
CO2 che rimuove l’aria dal dispositivo e dai tubi. Questa operazione
di spurgo richiede circa 10secondi e deve essere eseguita prima
di inserire il dispositivo monouso nella paziente onde evitare il
rischio di embolia gassosa. Sull’RFC modello 10 viene visualizzato
un messaggio relativo allo spurgo del dispositivo e viene emesso un
segnale acustico pulsante per tutta la procedura di spurgo. È possibile
inserire il dispositivo solo dopo che gli impulsi sonori cessano, la spia
non lampeggia più e i messaggi su schermo scompaiono.
• Per le pazienti portatrici di pacemaker o altri impianti di tipo attivo
sussiste il rischio di interferenza con il pacemaker e di danni allo stesso.
Consultare il produttore del pacemaker per ulteriori informazioni nel
caso in cui sia previsto il ricorso alla procedura NovaSure su pazienti
portatrici di pacemaker.
• Prestare attenzione affinché la paziente non entri a contatto con parti
metalliche messe a terra o che possiedano una notevole capacitanza
verso terra.
• Pericolo: rischio di esplosione. Da non usare in presenza di miscele
anestetiche infiammabili. Da non usare in presenza di gas o liquidi
infiammabili.
• Un guasto nel controller RF NovaSure può causare un aumento non
voluto dell’energia in uscita.

5
ITALIANO
Precauzioni
• La letteratura esistente riporta che le pazienti con un utero severamente
anteverso, retroflesso o posizionato lateralmente corrono un rischio
maggiore di perforazione della parete uterina durante qualsiasi
procedura intrauterina.
• Soprattutto in presenza di un utero severamente anteverso, retroflesso
o posizionato lateralmente, qualsiasi manipolazione dell’utero
comporta il rischio di un inserimento errato. Prestare attenzione per
assicurarsi che il dispositivo venga correttamente posizionato nella
cavità uterina.
• Il sistema NovaSure è costituito dai seguenti componenti:
- Dispositivo monouso NovaSure da usarsi su una singola paziente
erelativo cavo di collegamento
- e il controller RF NovaSure
- Contenitore per CO2 NovaSure
- Disidratante NovaSure
- Interruttore a pedale NovaSure
- Cavo di alimentazione
Per assicurare un corretto funzionamento del sistema, non usare
componenti diversi da quelli forniti con il sistema NovaSure.
Ispezionare regolarmente i componenti per escludere danni; non
utilizzarli in caso di danni evidenti. L’utilizzo di cavi o accessori diversi
da quelli specificati nelle presenti istruzioni potrebbe causare un
aumento delle emissioni o una ridotta immunità del controller RF.
• Per garantire la compatibilità elettromagnetica, il controller RF deve
essere installato e messo in servizio in accordo alle linee guida
fornite nelle presenti istruzioni. Consultare le tabelle su immunità ed
emissioni elettromagnetiche nella sezione Specifiche tecniche.
• Il controller RF non deve essere utilizzato in posizione adiacente o
sovrapposta ad altre apparecchiature. In caso di utilizzo in posizioni di
adiacenza o sovrapposizione, controllare il controller RF per verificare
il normale funzionamento nella configurazione in cui verrà utilizzato.
• Le apparecchiature con comunicazioni RF portatili e mobili possono
influire sul controller RF. Per le distanze di separazione consigliate,
consultare le tabelle sull’immunità elettromagnetica nella sezione
Specifiche tecniche.
• Le pazienti soggette ad ablazione endometriale e che in seguito
devono seguire una terapia ormonale sostitutiva dovranno
assumere anche progestina, onde evitare un aumento del rischio di
adenocarcinoma endometriale associato alla terapia di sostituzione a
base di solo estrogeno.
• La sicurezza e l’efficacia del sistema NovaSure non sono state
pienamente valutate nelle seguenti tipologie di pazienti:
- pazienti con una isterometria uterina maggiore di 10 cm;
- pazienti con fibromi sottomucosi che distorcono la cavità uterina;
- pazienti con utero bicorne, utero setto o subsetto;
- pazienti sottopostesi a trattamento preliminare di tipo medico
(adesempio agonista del GnRH, ormone di rilascio delle
gonadotropine) o chirurgico;
- pazienti che sono state precedentemente soggette ad ablazione
endometriale (inclusa un’ablazione con il sistema NovaSure);
- pazienti in post-menopausa.
• Non tentare di riparare il controller se si sospetta la presenza di
problemi. Per istruzioni su come procedere, contattare l’assistenza
tecnica o il rivenditore autorizzato Hologic.
• I cavi che portano al dispositivo monouso devono essere collocati
in modo tale da non entrare in contatto con la paziente né con altri
elettrodi.
• Prima dell’uso, ispezionare il dispositivo monouso per assicurarsi che
non sia danneggiato.
• Il disidratante della linea di suzione è non sterile e la sua confezione
non deve essere portata nel campo sterile.
• Se sullo schermo del modello 10 compare il messaggio “ARRAY
Position” (Posizione ARRAY), fare riferimento alla sezione “Risoluzione
dei problemi” alla voce “ALLARME POSIZIONE ARRAY”.
• Non usare il disidratante della linea di suzione NovaSure nel caso in
cui il disidratante abbia assunto una colorazione rosa.
• Collegare il cavo del dispositivo monouso all’apposita porta sul
pannello anteriore del controller prima di inserire il dispositivo nella
paziente (punto 2.15).
• Il contenitore di anidride carbonica contiene gas ad alta pressione. Se il
contenitore di CO2 o la linea si sono forati, attendere che il contenitore si
scarichi completamente, quindi lasciare che il contenitore e/o le linee si
equilibrino a temperatura ambiente prima di maneggiarli.
• La CO2 fluisce in modo ininterrotto dal momento in cui si collega
il dispositivo monouso al controller e fino al termine dell’esame di
valutazione dell’integrità della cavità. Per ridurre al minimo la durata
del flusso di CO2 e il conseguente rischio di embolia, posizionare il
dispositivo monouso immediatamente dopo averlo inserito ed eseguire
immediatamente l’esame.
• I conduttori elettrici (come gli elettrodi di monitoraggio di eventuali altri
dispositivi) che entrano in contatto diretto con l’array di elettrodi del
dispositivo monouso o si trovano in prossimità dello stesso possono
deviare una parte di corrente dall’array. Ne possono risultare ustioni
localizzate alla paziente o al medico così come la distorsione del
campo elettrico dell’array, che a sua volta modificherebbe l’efficacia
terapeutica (comportando un trattamento eccessivamente debole o
eccessivamente forte). Può anche causare la distorsione della corrente
nell’oggetto conduttore, ad esempio i monitor potrebbero visualizzare
valori inesatti.
• Una messa a terra affidabile è ottenibile solo quando l’attrezzatura è
collegata a una presa di categoria ospedaliera.
• Per evitare rischi per il paziente e gli operatori, non utilizzare questo
apparecchio in presenza di sorgenti magnetiche intenzionali, sorgenti
di ultrasuoni intenzionali o fonti di calore intenzionali.

6
ITALIANO
• Il collare cervicale deve essere completamente retratto in posizione
prossimale al fine di ridurre al minimo la possibilità di danni alla
guaina quando si chiude l’array.
• Il dispositivo NovaSure è controindicato in gravidanza o nelle donne
che stanno programmando una gravidanza. Le gravidanze dopo
l’ablazione possono essere pericolose sia per la madre sia per il feto.
Richiedere un giudizio medico accurato.
Dati clinici NovaSure a 3 anni
Effetti collaterali
Il sistema NovaSure è stato valutato in uno studio randomizzato,
prospettico e multicentrico che includeva 265 pazienti con sanguinamento
uterino anomalo; lo studio confrontava il sistema NovaSure con un gruppo
di controllo sottoposto a resezione dell’endometrio con ansa seguita da
ablazione con Rollerball.
Tabella 1A. Effetti collaterali intraoperatori
Effetti collaterali
NovaSure
n=175 (%)
Resezione con
ansa + rollerball
n=90 (%)
Bradicardia 1 (0,6%) 0 (0,0%)
Perforazione dell’utero 0 (0,0% 3 (3,3%)
Lacerazione cervicale 0 (0,0% 2 (2,2%)
Stenosi cervicale 0 (0,0% 1 (1,1%)
TOTALE 1 (0,6%) 6 (6,7%)
Tabella 1B. Effetti collaterali postoperatori <24 ore
Effetti collaterali
NovaSure
n=175 (%)
Resezione con
ansa + rollerball
n=90 (%)
Crampi/dolori pelvici 6 (3,4%) 4 (4,4%)
Nausea e/o vomito 3 (1,7%) 1 (1,1%)
TOTALE 9 (5,1%)* 5 (5,6%)**
* Nove eventi riportati in 6 (3,4%) pazienti
** Cinque eventi riportati in 4 (4,4%) pazienti
Tabella 1C. Effetti collaterali postoperatori >24 ore – 2 settimane
Effetti collaterali
NovaSure
n=175 (%)
Resezione con
ansa + rollerball
n=90 (%)
Ematometra 1 (0,6%) 0 (0,0%
Infezione del tratto urinario 1 (0,6%) 1 (1,1%)
Infezione vaginale 1 (0,6%) 0 (0,0%
Endometrite 0 (0,0% 2 (2,2%)
Malattia infiammatoria pelvica 0 (0,0% 1 (1,1%)
Emorragia 0 (0,0% 1 (1,1%)
Crampi/dolori pelvici 1 (0,6%) 1 (1,1%)
Nausea e/o vomito 1 (0,6%) 1 (1,1%)
Tabella 1C. Effetti collaterali postoperatori >24 ore – 2 settimane
TOTALE 5 (2,9%)* 7 (7,8%)**
* Cinque eventi riportati in 4 (2,3%) pazienti
** Sette eventi riportati in 6 (6,7%) pazienti
Tabella 1D. Effetti collaterali postoperatori >2 settimane – 1 anno
Effetti collaterali
NovaSure
n=175 (%)
Resezione con
ansa + rollerball
n=90 (%)
Isterectomia 3 (1,7%) 2 (2,2%)
Ematometra 1 (0,6%) 2 (2,2%)
Infezione del tratto urinario 2 (1,1%) 2 (2,2%)
Infezione vaginale 5 (2,9%) 2 (2,2%)
Endometrite 2 (1,1%) 1 (1,1%)
Malattia infiammatoria pelvica 2 (1,1%) 0 (0,0%
Emorragia 1 (0,6%) 0 (0,0%
Crampi/dolori pelvici 5 (2,9%) 6 (6,7%)
TOTALE 21 (12,0%)* 15 (16,17%)**
* 21 eventi riportati in 19 (10,9%) pazienti
** 15 eventi in 15 (16,7%) pazienti
Possibili complicanze postoperatorie
Per qualsiasi tipo di ablazione endometriale, sono stati documentati gli
eventi postoperatori delineati di seguito:
• Nelle prime 24 ore dopo la procedura, crampi e dolori pelvici sono
stati riferiti dal 3,4% delle pazienti NovaSure e dal 4,4% delle pazienti
trattate con resezione con ansa e ablazione con rollerball. I crampi
postoperatori variano da leggeri a molto forti e durano tipicamente
qualche ora; solo raramente continuano per più di un giorno dopo
laprocedura.
• Nelle prime 24 ore dopo la procedura, crampi e dolori pelvici sono stati
riferiti dall’1,7% delle pazienti NovaSure e dall’1,1% delle pazienti
soggette a resezione con ansa e ablazione con rollerball. Quando
insorgono, la nausea e il vomito si presentano in genere subito dopo
laprocedura, sono tipicamente associati all’anestesia e possono
essere trattati con farmaci.
• Secrezione vaginale
• Perdita ematica/stillicidio
Altri effetti collaterali
Come con qualsiasi procedura di ablazione endometriale, esiste la
possibilità di lesione grave e di decesso.
Gli effetti collaterali elencati di seguito potrebbero insorgere o sono stati
riferiti in associazione all’uso del sistema NovaSure:
• Sindrome da sterilizzazione delle tube post-ablazione
• Complicanze associate alla gravidanza (NOTA: LE GRAVIDANZE
CHE HANNO LUOGO DOPO UN’ABLAZIONE POSSONO ESSERE
RISCHIOSE PER LA MADRE E PER IL FETO)
• Lesioni termiche al tessuto adiacente

7
ITALIANO
• Perforazione della parete uterina
• Difficoltà di defecazione o minzione
• Necrosi uterina
• Embolia gassosa
• Infezione o sepsi
• Complicanze in grado di causare lesioni gravi o decesso
Studio clinico
Obiettivo: valutare la sicurezza e l’efficacia del sistema NovaSure al
confronto con la resezione endometriale con ansa seguita da ablazione
con rollerball nelle donne in pre-menopausa soggette a menorragia
associata a cause benigne.
Trattamento preliminare: le pazienti randomizzate nel gruppo NovaSure
non sono state sottoposte ad alcun trattamento preliminare dell’endometrio
(ad es. ormonale, D&C o raschiamento). Le pazienti randomizzate nel
gruppo di controllo sono state sottoposte, come trattamento preliminare, a
resezione con ansa.
Endpoint dello studio: quale fattore principale per misurare l’efficacia del
trattamento è stato utilizzato un sistema di valutazione del ciclo mestruale
a punteggio sviluppato da Higham (Higham JM, O’Brien PMS, Shaw RW Br
J Obstet Gynaecol 1990; 97:734-9). La valutazione della perdita ematica
mestruale è stata eseguita usando un grafico PBLAC (Pictorial Blood
Loss Assessment Chart, grafico illustrato della valutazione della perdita
ematica mestruale). Il trattamento veniva considerato riuscito quando a
1anno dalla procedura si otteneva una riduzione del flusso mestruale tale
da assegnare al flusso un punteggio <75. Si considerava che lo studio
clinico avesse esito positivo quando la differenza statistica tra il tasso di
successo tra le pazienti soggette a trattamento con il sistema di ablazione
endometriale NovaSure a impedenza e il tasso di successo tra le pazienti
soggette a resezione con ansa e ablazione con rollerball era inferiore al
20%. Le pazienti sono state contattate a due e tre anni dall’intervento
per rispondere ad alcune domande relative al sanguinamento negli ultimi
12mesi. Lo stato di sanguinamento di ciascuna paziente è stato valutato
a due e a tre anni dall’intervento avvalendosi del punteggio PBLAC e di un
modello di sanguinamento usato come riferimento. In tal modo, è stato
possibile eseguire un confronto diretto tra il pattern di sanguinamento o
lostato mestruale di una paziente a un anno, a due e a tre anni.
Gli endpoint secondari includevano il regime anestetico, la durata della
procedura e le risposte fornite tramite un questionario sulla qualità
di vita. La sicurezza è stata valutata sulla base degli effetti collaterali
documentati durante lo studio.
Metodi: è stato condotto uno studio clinico randomizzato (2:1) prospettico
in 9 centri per un totale di 265 pazienti con diagnosi di menorragia.
Ipunteggi relativi alle mestruazioni sono stati raccolti prima dell’intervento
e poi ogni mese per 12 mesi dopo l’intervento. Il trattamento poteva
avere luogo in qualsiasi momento del ciclo mestruale. Nessuna delle
pazienti è stata trattata preliminarmente con trattamento ormonale per
rendere più sottile l’endometrio. Le pazienti nel gruppo di controllo sono
state sottoposte a resezione isteroscopica con ansa come trattamento
preliminare e quindi ad ablazione con rollerball. Per selezionare le pazienti
da includere nello studio sono stati utilizzati i requisiti indicati di seguito:
Criteri di inclusione
• Menorragia refrattaria senza una causa organica definita
(sanguinamento uterino disfunzionale)
• Età compresa tra 25 e 50 anni
• Dimensioni dell’utero tra 6 e 10 cm (dall’orifizio esterno del collo
dell’utero al fondo uterino)
• Punteggio PBLAC minimo >150 per i 3 mesi antecedenti alla
partecipazione allo studio oppure punteggio PBLAC >150 per un
mesenel caso di donne che:
- siano state sottoposte per almeno 3 mesi (documentabili) antecedenti
allo studio a terapia medica non riuscita;
- presentino una condizione per la quale è controindicata la terapia
medica;
- abbiano rifiutato la terapia medica.
Criteri di esclusione
• Presenza di batteriemia, sepsi o altra infezione sistemica attiva
• Malattie infiammatorie pelviche attive o ricorrenti
• Pazienti con coagulopatie documentate o sottopostesi a terapie
anticoagulanti
• Endometriosi sintomatica
• Pregresso intervento all’utero (ad eccezione del taglio cesareo con
incisione bassa) che compromette l’integrità della parete uterina, ad
esempio la miomectomia transmurale o un taglio cesareo tradizionale
• Precedente ablazione endometriale
• Pazienti trattate con farmaci in grado di assottigliare il muscolo
miometriale (ad es. un uso prolungato di steroidi)
• Pazienti che desiderano avere altre gravidanze o mantenere la fertilità
• Pazienti che attualmente usano un metodo anticoncezionale ormonale
e non intendono usare un metodo non ormonale dopo l’ablazione
• Cavità anomala od ostruita, come confermato con una isteroscopia
SONOGRAFIA CON SOLUZIONE SALITA (SIS) oppure
ISTEROSALPINOGRAFIA (HSG). In particolare:
- utero setto o bicorne o altra malformazione congenita della cavità
uterina
- fibromi sottomucosi con peduncoli o altri tipi di fibroma che causano
una distorsione della cavità; polipi (superiori a 2 cm) suscettibili di
causare una menorragia
- presenza di una spirale
• Neoplasia sospetta o confermata negli ultimi cinque anni, confermata
con esame istologico
• Iperplasia endometriale confermata con esame istologico
• Displasia cervicale non curata
• Livelli di FSH (ormone follicolo-stimolante) alti come nella menopausa
>40 UI/ml
• Gravidanza
• Malattia venerea attiva

8
ITALIANO
Popolazione pazienti: hanno partecipato allo studio 265 pazienti di
età compresa tra i 25 e i 50 anni (con il 46% di età inferiore ai 40anni
e il 54% di età pari o superiore ai 40 anni). Non vi era differenza nei
parametri demografici o nell’anamnesi ginecologica tra i gruppi di
trattamento, tra i gruppi di età o tra i nove diversi centri che hanno preso
parte allo studio.
Tabella 2. Organizzazione delle pazienti
Numero delle pazienti NovaSure Resezione ad
ansa + Rollerball
Ammissione allo studio
(popolazione Intent-to-Treat) 175 90
Procedure interrotte*1-4 -2
Trattate 171 88
Trattamento addizionale* -4 -2
Isterectomia*2-3 -2
Mai presentate al follow-up* -5 -2
Malattia di Hodgkin* -1 0
Dolore pelvico - leuprolide somministrato* -1 0
Dati disponibili al follow-up a 12 mesi 157 82
Trattamento addizionale* -2 -1
Isterectomia*2-3 -1
Mai presentate al follow-up* -2 -5
Hanno mancato una visita -1 -1
Non hanno voluto partecipare* -1 0
Gravidanza* -1 0
Dati disponibili al follow-up a 24 mesi 147 74
Trattamento addizionale* 0 -4
Isterectomia*2-5 -1
Mai presentate al follow-up* -4 -2
Follow-up a 36 mesi 138 67
Il soggetto non si è presentato al
follow-up di 24 mesi ma è tornato
per la visita dei 36 mesi
+1 +1
Dati disponibili al follow-up a 36 mesi 139 68
* Pazienti rimosse dallo studio
1 Quattro pazienti NovaSure non presentavano i criteri necessari per l’inclusione; due pazienti soggette a
trattamento con rollerball presentavano una perforazione dell’utero
2 Per ulteriori informazioni sull’isterectomia, vedere la Tabella 7
Risultati
Endpoint primario per la determinazione dell’efficacia:
punteggio di sanguinamento
L’intervento viene considerato riuscito a 12 mesi dalla procedura, se il
punteggio presenta una riduzione da un punteggio >150 prima della
procedura a un punteggio <75 dopo la procedura. L’amenorrea viene
definita come un punteggio di 0. Ai 24 e 36 mesi, secondo i sondaggi
telefonici condotti, un intervento viene considerato riuscito se il
sanguinamento viene eliminato o comunque ridotto a un flusso leggero
o normale. La Tabella 3 di seguito contiene i risultati clinici relativi al
totale delle 265 pazienti randomizzate (gruppo Intent-to-Treat, ITT) ai fini
dello studio. I risultati peggiori si otterrebbero considerando le pazienti
rimosse dallo studio (incluse nella Tabella 2) come “interventi non
riusciti” ai fini del calcolo dei valori elencati nella tabella.
Tabella 3. Efficacia: Tasso di successo–Pazienti Intent-To-Treat
NovaSure
(n=175)
Resezione ad
ansa + Rollerball
(n=90)
Mesi dopo l’intervento
di ablazione
12* 24** 36** 12* 24** 36**
Numero di pazienti
con intervento riuscito
136 143 134 67 68 63
Percentuale di esiti
riusciti
77,7% 81,7% 76,6% 74,4% 75,6% 70,0%
N. di pazienti con
amenorrea
63 64 58 29 26 23
Percentuale di
amenorrea
36,0% 36,6% 33,1% 32,2% 28,9% 25,6%
* Sulla base dei punteggi
** Sulla base dei sondaggi effettuati telefonicamente
Endpoint secondario per la determinazione dell’efficacia:
qualitài vita
Per determinare la qualità di vita della paziente (QOL) ci si è avvalsi del
questionario sulla qualità di vita (SF-12) e del questionario sull’impatto
mestruale compilato prima del trattamento e a 3, 6, 12, 24 e 36 mesi
dalla procedura. La Tabella 4 illustra le risposte delle pazienti per
entrambi i gruppi, in fase preoperatoria, quando appropriato, e a 12,
24e36 mesi dalla procedura.
Tabella 4. Efficacia: Qualità di vita (QOL)
NovaSure Resezione ad
ansa + Rollerball
Numero di pazienti che hanno risposto al sondaggio
#
sulla qualità della vita
Preoperatoria 175 90
12 mesi 154 82
24 mesi 143 73
36 mesi 139 67
Percentuale di pazienti soddisfatte o molto soddisfatte
12 mesi 92,8% 93,9%
24 mesi 93,9% 89,1%
36 mesi 96,3% 89,7%
Percentuale di pazienti che probabilmente o sicuramente raccomanderebbero
l’intervento
12 mesi 96,7% 95,9%
24 mesi 96,6% 94,5%
36 mesi 97,8% 92,6%
Percentuale di pazienti con dismenorrea
Preoperatoria 57,1% 55,6%
12 mesi 20,8%& 34,2%*,&
24 mesi 20,3%* 30,1%*
36 mesi 17,3%* 28,4%*
Percentuale di pazienti con sindrome premestruale
Preoperatoria 65,1% 66,7%
12 mesi 36,4%* 35,4%*
24 mesi 44,0%* 46,6%*
36 mesi 34,5%* 41,2%*

9
ITALIANO
Tabella 4. Efficacia: Qualità di vita (QOL)
NovaSure Resezione ad
ansa + Rollerball
Percentuale di pazienti che riferiscono problemi di natura sporadica,
frequente o costante nell’eseguire il proprio lavoro o altre attività a
causa delle mestruazioni
Preoperatoria 66,3% 65,5%
12 mesi 9,9%* 8,6%*
24 mesi 14,5%* 15,0%*
36 mesi 16,3%* 13,3%*
Percentuale di pazienti che riferiscono problemi di ansia di natura
sporadica, frequente o costante a causa delle mestruazioni
Preoperatoria 74,7% 68,9%
12 mesi 23,6%* 18,5%*
24 mesi 24,2%* 19,2%*
36 mesi 18,7%* 19,1%*
Percentuale di pazienti che riferiscono di dover rinunciare a eventi sociali
su base sporadica, frequente o costante a causa delle mestruazioni
Preoperatoria 63,3% 62,2%
12 mesi 8,5%* 8,6%*
24 mesi 9,0%* 11,1%*
36 mesi 8,1%* 10,8%*
# Non tutte le pazienti hanno completato il sondaggio
* Differenza statisticamente significativa dalla risposta in fase preoperatoria (chi al quadrato; p<0,05)
& Differenza notevole da un punto di vista statistico tra i due gruppi NovaSure e Rollerball
(chi al quadrato; p=0,02)
Endpoint di sicurezza
I dati relativi agli effetti collaterali sono riportati nella sezione “Effetti
collaterali” del presente manuale.
Endpoint secondario: tempo della procedura
Il tempo della procedura, un endpoint secondario, è stato determinato
annotando per ogni paziente il tempo di inserimento e di rimozione del
dispositivo. Il tempo medio della procedura per le pazienti NovaSure
è stato notevolmente inferiore rispetto al tempo della procedura per il
gruppo Rollerball (4,2 ± 3,5 minuti e 24,2 ± 11,4 minuti, rispettivamente).
I tempi medi di applicazione dell’energia in radiofrequenza sono stati di
84,0 ±25,0secondi in un sottogruppo di pazienti NovaSure controllate
(Tabella5).
Tabella 5. Tempo della procedura
Parametri operativi NovaSure
n=175
Resezione ad
ansa + Rollerball
n=90
Numero di pazienti trattate* 171 88
Tempo della procedura in minuti (± DS)
(dall’inserimento alla rimozione del
dispositivo)
4,2 ± 3,5** 24,2 ± 11,4**
Tabella 5. Tempo della procedura
Tempo della procedura in secondi (± DS)
(tempo di erogazione dell’energia)
84,0 ± 25,0 ND#
* Per l’organizzazione delle pazienti, vedere la Tabella 2
** Differenza notevole dal punto di vista statistico tra i gruppi di trattamento (distribuzione di Student;
p <0,05)
# Non determinato
Endpoint secondario: regime di anestesia
La scelta dell’anestesia è stata effettuata da ciascuna paziente
unitamente al ricercatore e all’anestesista di turno. Il 27% (47/174)
delle pazienti NovaSure ha subito l’intervento in anestesia generale
o epidurale e il 73% (127/174) in anestesia locale o con sedativi
somministrati per via endovenosa. Per una paziente di questo gruppo
non è stato riferito il regime di anestesia. Nel gruppo Rollerball, l’82,2%
(74/90) delle pazienti è stato trattato in anestesia generale o epidurale e
il 17,8% (16/90) in anestesia locale o con sedativi somministrati per via
endovenosa (Tabella 6).
Tabella 6. Regime di anestesia
NovaSure
n=175*
Resezione ad
ansa + Rollerball
n=90
Generale o epidurale 27,0% 82,2%
Locale e/o sedativi per via endovenosa 73,0% 17,8%
* Per una paziente il regime di anestesia non è stato riferito.
Osservazioni cliniche
Isterectomia
Quindici donne sono state sottoposte a isterectomia nei tre anni
successivi alla procedura. La Tabella 7 indica i motivi per l’isterectomia.
Tabella 7. Isterectomia
Motivi per l’isterectomia NovaSure
n=175
Resezione ad
ansa + Rollerball
n=90
Adenocarcinoma diagnosticato al
momento dell’ablazione 1 1
Fibromi 2 0
Ascesso pelvico 1 1
Endometriosi 3 0
Adenomiosi 4 0
Ematometra 0 1
Menorragia 0 1
TOTALE 11 (6,3%) 4 (4,4%)
7 isterectomie eseguite su pazienti con meno di 40 anni (delle quali 7 pazienti NovaSure) e 8 isterectomie
eseguite su pazienti con più di 40 anni (4 NovaSure; 4 Rollerball).
Selezione delle pazienti
La menorragia può essere causata da una varietà di problemi secondari
tra cui tumore dell’endometrio, mioma, polipi, farmaci e sanguinamento
uterino disfunzionale (sanguinamento anovulatorio). È necessario
eseguire uno screening delle pazienti e valutarle onde determinare
la causa dell’eccessivo sanguinamento uterino prima di avviare un
trattamento. Fare riferimento alla letteratura medica relativa all’ablazione
endometriale e consultare tecniche, indicazioni, controindicazioni,
complicanze e rischi prima di eseguire una procedura.

10
ITALIANO
Consulenza alle pazienti
Come con qualsiasi tipo di procedura, il medico deve discutere i rischi,
i vantaggi e le alternative con la paziente prima di eseguire l’ablazione
endometriale. Le aspettative della paziente devono essere realistiche e
la paziente deve comprendere che lo scopo del trattamento è di ridurre
ilsanguinamento e portarlo a livelli normali.
Il dispositivo monouso deve essere usato esclusivamente sulle donne
che non desiderano avere altre gravidanze, poiché la possibilità di una
gravidanza risulta molto diminuita dopo la procedura. Le pazienti fertili
devono essere avvisate che, nel caso di una gravidanza in seguito
all’ablazione, potrebbero insorgere complicanze. Durante la consulenza
alla paziente, discutere del metodo contraccettivo da usare dopo
l’intervento, se necessario. Questa procedura non è una procedura di
sterilizzazione ed eventuali gravidanze successive all’intervento possono
comportare rischi per la madre e per il feto.
Nel corso delle prime settimane successive all’ablazione sono possibili
secrezioni vaginali, che possono perdurare fino a un mese. Tipicamente,
queste secrezioni sono di carattere ematico nei primi cinque giorni,
sieroematiche intorno alla prima settimana e quindi profuse e acquose.
Eventuali secrezioni atipiche o maleodoranti devono essere riferite
immediatamente al medico. Altre complicanze comuni in seguito
all’intervento includono crampi e dolori pelvici, nausea e vomito.
La perforazione dell’utero deve essere considerata nella diagnosi
differenziale di una paziente postoperatoria che accusa dolori addominali
acuti, febbre, mancanza di respiro, giramenti di testa, ipotensione o altri
sintomi potenzialmente associati con la perforazione dell’utero con o
senza lesioni agli organi adiacenti della cavità addominale. Le pazienti
devono essere avvisate che eventuali sintomi di questo tipo vanno riferiti
immediatamente al medico.
Preparazione della paziente all’intervento
Il sistema di ablazione endometriale NovaSure a impedenza è in grado
di trattare una cavità uterina con spessore endometriale compreso in un
dato intervallo. Il rivestimento dell’utero non deve essere assottigliato
prima della procedura e l’intervento può essere eseguito durante la fase
proliferativa o secretoria del ciclo. Sebbene la sicurezza e l’efficacia
del sistema NovaSure non siano state valutate appieno per pazienti
sottopostesi a trattamento preliminare di tipo medico o chirurgico, il
sistema è stato però valutato su un numero limitato di pazienti pretrattate
con agonisti del GnRH e non ha mostrato complicanze o effetti collaterali.
Un sanguinamento attivo non è da ritenersi una controindicazione all’uso
del sistema NovaSure. Si raccomanda di somministrare un farmaco
antinfiammatorio non steroideo da prendere almeno un’ora prima del
trattamento e quindi successivamente all’intervento per ridurre i crampi
all’utero intra e postoperatori.
Sistema di ablazione endometriale NovaSure a impedenza
Istruzioni per l’uso
Prima dell’uso, leggere le istruzioni, le avvertenze e le precauzioni.
1.0 Allestimento
CONTROLLER RF
NOVASURE
DISPOSITIVO MONOUSO NOVASURE
CON CAVO DI COLLEGAMENTO,
INCLUSO IL DISIDRATANTE DELLA
LINEA DI SUZIONE
CAVO DI ALIMENTAZIONE
NOVASURE
DISIDRATANTE DELLA LINEA
DI SUZIONE NOVASURE
CONTENITORE NOVASURE CO2
Lorem ipsum
INTERRUTTORE A PEDALE
NOVASURE
1.1 Per usare il sistema NovaSure sono necessari:
• un dispositivo monouso NovaSure sterile per uso su una singola
paziente con
• un cavo di collegamento
• un controller RF NovaSure
• un interruttore a pedale NovaSure
• un cavo di alimentazione c.a. NovaSure
• un disidratante della linea di suzione NovaSure non sterile
• un contenitore per CO2 NovaSure
Valvola di sfiato
del vuoto
Collare cervicale
Array di elettrodi
bipolari
Impugnatura anteriore
Guaina
Impugnatura
posteriore
Linea di
suzione
Pulsante di
rilascio
Impostazione della lunghezza della cavità
Punta della
linea del vuoto
selettore WIDTH
(LARGHEZZA)

11
ITALIANO
Nota: tenere a disposizione almeno un dispositivo monouso, un
gruppo con disidratante e un contenitore per CO2 di scorta.
1.2 Preparare il controller RF NovaSure. Posizionarlo su un tavolino
a lato della paziente e all’interno del campo visivo del chirurgo.
Collegare il cavo di alimentazione al controller e inserirlo in una
presa di corrente.
1.3 Fissare il contenitore per CO2 sul regolatore posto sul pannello
posteriore del controller.
1.4 Ruotare completamente la manopola (se disponibile) di regolazione
della CO2 portandola nella posizione alta (HI).
Nota: i modelli di controller più recenti non sono provvisti di
manopola sul regolatore e pertanto il flusso di CO2 viene regolato
automaticamente. Nel caso in cui il controller non sia provvisto di
manopola per il regolatore, procedere al punto 1.5.
1.5 Portare l’interruttore posto sul pannello posteriore del controller in
posizione ON (ACCESO).
1.6 Collegare l’interruttore a pedale all’apposita porta sul pannello
frontale del controller.
Nota: all’accendere per la prima volta il controller RF modello
10 viene visualizzata la schermata “Selezionare la lingua”.
L’impostazione predefinita è la lingua inglese. Per selezionare una
lingua diversa, premere il pulsante associato alla lingua desiderata.
Salvare la scelta effettuata premendo il pulsante verde lampeggiante.
La scelta della lingua viene così memorizzata. Per modificare la lingua
dopo l’impostazione iniziale, usare la schermata “Impostazioni”.
Per cambiare la lingua di visualizzazione delle schermate, premere
il nome della lingua di interesse. Per salvare le modifiche apportate
alle impostazioni, premere il pulsante verde lampeggiante.
Per annullare una selezione effettuata, premere la “X” blu.
2.0 Procedura
2.1 Preparare la paziente per l’anestesia.
2.2 Mettere la paziente in posizione di litotomia dorsale.
Porta
2.3 Anestetizzare la paziente conformemente alle pratiche standard.
2.4 Eseguire un’esplorazione a due mani. Valutare la posizione
dell’utero e determinare se sia severamente anteverso o retroverso.
2.5 Preparare la paziente e coprirla con un telo come per una
procedura di dilatazione e raschiamento.
2.6 Inserire lo speculum nella vagina.
2.7 Afferrare la cervice con un uncino.
2.8 Misurare la lunghezza dell’utero dal fondo uterino all’orifizio esterno
del collo dell’utero. L’efficacia del sistema NovaSure non è stata
valutata appieno nelle pazienti con un utero maggiore di 10 cm.
2.9 Determinare la lunghezza del canale cervicale e dilatare il
canale per l’inserimento del dispositivo.
NOTA: il diametro nominale del dispositivo monouso NovaSure
è di 6 mm.
2.10 Consultare la tabella relativa alla lunghezza della cavità (vedere
sotto) per le impostazioni corrette sulla base delle misurazioni
effettuate dell’utero e del canale cervicale. Negli intervalli più alti,
le dimensioni sono state modificate per riflettere la lunghezza
dell’elettrodo del dispositivo monouso.
La corretta determinazione della lunghezza della cavità uterina è
essenziale per garantire un trattamento sicuro ed efficace. Una
stima per eccesso della lunghezza della cavità può comportare
lesioni termiche al canale endocervicale.
Avvertenza: prestare attenzione a non perforare la parete
uterina durante la misurazione, la dilatazione o l’inserimento del
dispositivo monouso.
TABELLA 8. LUNGHEZZA DELLA CAVITÀ
Sonda uterina (cm)
Lunghezza
della cervice
(cm) 10 9,5 9 8,5 8 7,5 7 6,5 6
26,5* 6,5* 6,5* 6,5 6 5,5 5 4,5 4
2,5 6,5* 6,5* 6,5 6 5,5 5 4,5 4
36,5* 6,5 6 5,5 5 4,5 4
3,5 6,5 6 5,5 5 4,5 4
46 5,5 5 4,5 4
4,5 5,5 5 4,5 4
55 4,5 4
5,5 4,5 4
64
* Il valore di 6,5 non riflette la differenza numerica tra la lunghezza della sonda e la lunghezza del canale
cervicale.
Il valore 6,5 è stato invece inserito in quanto rappresenta la lunghezza massima che l’array NovaSure
puòraggiungere.
Controindicazioni: non trattare una paziente con una cavità uterina
di lunghezza inferiore ai 4 cm, poiché esiste il rischio di danni al
canale cervicale.
Sistema di ablazione endometriale NovaSure a impedenza
Istruzioni per l’uso
Prima dell’uso, leggere le istruzioni, le avvertenze e le precauzioni.
1.0 Allestimento
CONTROLLER RF
NOVASURE
DISPOSITIVO MONOUSO NOVASURE
CON CAVO DI COLLEGAMENTO,
INCLUSO IL DISIDRATANTE DELLA
LINEA DI SUZIONE
CAVO DI ALIMENTAZIONE
NOVASURE
DISIDRATANTE DELLA LINEA
DI SUZIONE NOVASURE
CONTENITORE NOVASURE CO2
Lorem ipsum
INTERRUTTORE A PEDALE
NOVASURE
1.1 Per usare il sistema NovaSure sono necessari:
• un dispositivo monouso NovaSure sterile per uso su una singola
paziente con
• un cavo di collegamento
• un controller RF NovaSure
• un interruttore a pedale NovaSure
• un cavo di alimentazione c.a. NovaSure
• un disidratante della linea di suzione NovaSure non sterile
• un contenitore per CO2 NovaSure
Valvola di sfiato
del vuoto
Collare cervicale
Array di elettrodi
bipolari
Impugnatura anteriore
Guaina
Impugnatura
posteriore
Linea di
suzione
Pulsante di
rilascio
Impostazione della lunghezza della cavità
Punta della
linea del vuoto
selettore WIDTH
(LARGHEZZA)
Interruttore
Contenitore CO2
Cavo di
alimentazione c.a.

12
ITALIANO
Nota: per le pazienti aventi una cavità uterina di lunghezza
superiore a 6 cm il tasso di successo è stato inferiore al tasso di
successo medio dell’intervento.
2.11 Aprire la confezione sterile del dispositivo monouso NovaSure. Porre
il dispositivo monouso con relativo cavo di collegamento nel campo
sterile, prestando attenzione a mantenere il disidratante della linea
di suzione non sterile al di fuori del campo sterile.
Avvertenza: non usare il dispositivo monouso sterile, se la confezione
appare danneggiata o se presenta segni di manomissione.
2.12 Aprire la confezione e il sigillo del disidratante della linea di suzione
non sterile. Rimuovere i tappi rossi.
Attenzione: il disidratante della linea di suzione è non sterile e la
sua confezione non deve essere portata nel campo sterile.
Attenzione: se il disidratante è di colore rosa, sostituirlo prima di
iniziare la procedura.
2.13 Collegare il disidratante alle punte presenti sul tubo di suzione del
dispositivo monouso. Assicurarsi che le punte siano completamente
inserite nei tubi del disidratante.
2.14 Attenzione: prima di eseguire l’operazione indicata al
punto2.15, il dispositivo monouso non deve essere inserito
nella paziente.
2.15 Collegare il cavo del dispositivo monouso all’apposita porta sul
pannello frontale del controller.
Dispositivo monouso
Porta
Avvertenza: quando si inserisce il dispositivo monouso NovaSure nel
controller, ha inizio il flusso di CO2 che rimuove l’aria dal dispositivo
e dai tubi. L’operazione di spurgo richiede circa 10 secondi e deve
essere eseguita prima di inserire il dispositivo monouso nella
paziente. Sull’RFC modello 10 viene visualizzato un messaggio
relativo allo spurgo del dispositivo e viene emesso un segnale
acustico pulsante per tutta la procedura di spurgo.Quando il segnale
acustico (bip) cessa, la spia non lampeggia più e i messaggi su
schermo scompaiono, è possibile inserire il dispositivo monouso
NovaSure.
Attenzione: la CO2 fluisce in modo ininterrotto dal momento in cui
si collega il dispositivo monouso al controller e fino al termine
dell’esame di valutazione dell’integrità della cavità. Per ridurre
al minimo la durata del flusso di CO2 e il conseguente rischio di
embolia, posizionare il dispositivo monouso immediatamente dopo
averlo inserito ed eseguire immediatamente l’esame.
Avvertenza: prestare attenzione a non perforare la parete
uterina durante la misurazione, la dilatazione o l’inserimento del
dispositivo monouso.
2.16 Dispiegare il dispositivo monouso esternamente alla paziente e
assicurarsi che il messaggio su schermo non sia visualizzato sull’RFC
modello 10 all’apertura dell’array. Se il messaggio su schermo rimane
visualizzato sull’RFC modello 10, chiudere e riaprire il dispositivo
monouso. Se il problema persiste, sostituire il dispositivo monouso.
2.17 Assicurarsi che il selettore WIDTH (LARGHEZZA) indichi una
larghezza maggiore ouguale a 4 cm.
Selettore
WIDTH (LARGHEZZA)
Nota: se il selettore WIDTH (LARGHEZZA) mostra una misura inferiore
a 4cm, chiudere il dispositivo monouso e ripetere quanto indicato
precedentemente al punto 2.16. Se il selettore WIDTH (LARGHEZZA)
continua a indicare una larghezza inferiore ai 4 cm, usare un nuovo
dispositivo monouso e restituire l’altro al servizio di assistenza
tecnica di Hologic.
2.18 Sbloccare il dispositivo monouso premendo il pulsante di rilascio.
Chiudere il dispositivo monouso tenendo fermo il perno anteriore e
tirare lentamente indietro le impugnature posteriori fino a quando
l’apposita spia, posizionata sui cardini delle impugnature anteriore e
posteriore, indica “ARRAY CLOSED” (ARRAY CHIUSO). Questa indica
che l’array è stato retratto nella guaina del dispositivo monouso in
posizione di chiusura.

13
ITALIANO
Indicatore
ARRAY CLOSED
(ARRAY CHIUSO)
Pulsante di
rilascio
2.19 Assicurarsi che l’array sia completamente racchiuso dalla guaina
esterna.
2.20 Controllare che il selettore WIDTH (LARGHEZZA) indichi una larghezza di
circa 0,5 cm.
2.21 Sulla base delle misurazioni effettuate dell’utero e del canale
cervicale, consultare la tabella relativa alla lunghezza della cavità
(vedere sopra) per le impostazioni corrette di lunghezza della cavità,
come descritto sopra al punto 2.10.
Controindicazioni: non trattare una paziente con una cavità uterina
di lunghezza inferiore ai 4 cm, poiché esiste il rischio di danni al
canale cervicale.
2.22 Con l’ausilio della tabella relativa alla lunghezza della cavità nella
sezione 2.10, selezionare il valore ottenuto per la lunghezza nella
schermata di immissione dati del controller RF NovaSure premendo
le frecce su/giù.
2.23 Sul dispositivo monouso, regolare e bloccare l’impostazione relativa
alla lunghezza della cavità sul valore ottenuto sopra (vedere il
punto2.21). Assicurarsi che il collare cervicale sia completamente
retratto in posizione prossimale.
2.24 Confermare che la cervice sia dilatata di almeno 6 mm (il diametro
nominale del dispositivo monouso NovaSure).
2.25 Mantenere una leggera trazione sull’uncino per ridurre al minimo
l’angolo dell’utero.
2.26 Durante l’inserimento transcervicale nella cavità uterina, orientare
il dispositivo monouso affinché sia in linea con l’asse dell’utero.
Tenendo fermo il perno anteriore, far avanzare il dispositivo monouso
fino a quando l’estremità distale della guaina tocca il fondo.
#10
Lorem ipsum
Avvertenza: se l’inserimento del dispositivo monouso nel canale
cervicale risulta difficile, determinare sulla base della
propria esperienza se sia necessario dilatare ulteriormente.
2.27 Rimuovere il dispositivo monouso di circa 0,5 cm dal fondo uterino.
Premere lentamente le impugnature (SENZA BLOCCARLE) fino al
punto in cui aumenta la resistenza.
Il selettore WIDTH (LARGHEZZA) deve indicare una larghezza di
circa 0,5 cm. Aquesto punto la guaina è stata retratta.
0,5 cm

14
ITALIANO
2.28 Continuare a premere lentamente le impugnature del dispositivo
monouso e al contempo spostare con cautela il dispositivo avanti e
indietro di circa 0,5 cm dal fondo, ruotando l’impugnatura di 45° in
senso antiorario e di 45° in senso orario rispetto al piano verticale,
fino a quando le impugnature si bloccano.
Il selettore WIDTH (LARGHEZZA) deve indicare una larghezza
maggiore di 2,5 cm.
Nota: una volta che le impugnature del dispositivo monouso sono
bloccate, l’utero deve spostarsi unitamente al dispositivo.
2.29 Spostare delicatamente il dispositivo monouso con movimenti in
avanti, indietro e laterali.
2.30 Per completare il posizionamento, retrarre leggermente il dispositivo
monouso fino a quando il selettore WIDTH (LARGHEZZA) indica una
riduzione della larghezza di circa 0,2–0,5 cm.
2.31 Tenere l’uncino e far avanzare lentamente e delicatamente il
dispositivo monouso contro il fondo. Il selettore WIDTH (LARGHEZZA)
deve indicare una larghezza maggiore o uguale alla misurazione
precedente.
2.32 Far scivolare il collare cervicale in avanti premendo delicatamente
sulla linguetta del collare cervicale, in modo da formare un sigillo
contro l’orifizio esterno del collo dell’utero.
2.33 Leggere la misurazione tra corni (2,5 cm minimo) sul selettore WIDTH
(LARGHEZZA).
Controindicazioni: non trattare pazienti con una cavità uterina
di larghezza inferiore a 2,5 cm, secondo quanto determinato
dall’apposito selettore WIDTH (LARGHEZZA) del dispositivo monouso,
una volta che quest’ultimo è stato posizionato e dispiegato.
Attenzione: se appare l’avviso ARRAY POSITION (POSIZIONE
ARRAY), consultare “SPIA ARRAY POSITION” nella sezione relativa
alla risoluzione dei problemi.
2.34 Usando le apposite frecce su/giù, selezionare il valore indicato dal
selettore WIDTH (LARGHEZZA) nella schermata di immissione dati
sul controller RF NovaSure.
2.35 Il sistema può essere messo in funzione in modalità automatica
o manuale. In modalità automatica, il ciclo di ablazione verrà
avviato automaticamente al completamento corretto dell’esame di
valutazione. In modalità manuale, il ciclo di ablazione non si avvierà
automaticamente dopo il corretto completamento dell’esame di
valutazione.
Pressione leggera
Pressione forte

15
ITALIANO
nota: la collocazione corretta dell’array di elettrodi contro il fondo dell’utero è essenziale per garantire un trattamento sicuro ed efficace. Se
una porzione dell’array di elettrodi o il bordo distale della guaina esterna rimane nel canale endocervicale durante il trattamento, il rischio
di lesione termica endocervicale aumenta.
Fondo
Array di elettrodi
Bordo della guaina
Canale endocervicale
Il bordo della guaina si trova
nella parte bassa dell’utero
Array di elettrodi
Canale endocervicale Bordo della guaina
Il bordo della guaina rimane
nel canale endocervicale
Fondo
COLLOCAZIONE NON CORRETTA COLLOCAZIONE CORRETTA

16
ITALIANO
Funzionamento del controller RF modello 10
A. Modalità automatica
Per usare il controller RF modello 10, premere il pulsante “Cambia
modalità” quando questo appare nella parte inferiore dello
schermo. Procedere con le indicazioni del punto 2.36, ma non
seguire il punto2.37 se il funzionamento del sistema è in modalità
automatica.
B. Modalità manuale
Nota: la modalità manuale è l’impostazione predefinita del
sistema.
Per usare il sistema in modalità manuale, non premere il pulsante
“Cambia modalità” prima di iniziare l’esame di valutazione
dell’integrità della cavità uterina. Seguire le indicazioni dei
punti2.36 e 2.37.
2.36 Avviare la procedura di valutazione dell’integrità della cavità
premendo una volta l’interruttore a pedale. Sullo schermo viene
visualizzato il messaggio “Esame cavità in corso” mentre cinque
pallini che appaiono sullo schermo si accendono e spengono in
maniera sequenziale. La durata dell’esame varia da 7 a 30secondi
circa. Quando l’esame è completato con esito positivo, viene
visualizzato il messaggio “Esame cavità completato” e il sistema
è pronto a erogare energia in radiofrequenza. Non è possibile
attivare il dispositivo monouso finché non viene visualizzato questo
messaggio indicando il completamento dell’esame della cavità.
Nel caso in cui l’esame non viene superato, viene visualizzato
il messaggio “Esame cavità non riuscito” unitamente alla
procedura da seguire per risolvere il problema.
A. Se si sospetta una perforazione, terminare immediatamente
laprocedura.
B. Se anche questa volta l’esame non viene superato, controllare
che non vi siano perdite nel sistema o tra la cervice e il collare
cervicale. Controllare tutti i tubi e verificare che sia stata
installata una linea di suzione con disidratante. Se sussiste una
perdita in prossimità della cervice che non può essere risolta con
il collare cervicale, usare un altro uncino per avvolgere la cervice
intorno allaguaina. Ripetere l’esame premendo l’interruttore a
pedale.
Nota: in presenza di una cervice eccessivamente dilatata, è
possibile che abbia luogo una perdita di CO2 in corrispondenza
dell’orifizio esterno del collo dell’utero. In queste condizioni la
perdita di CO2 può essere accompagnata dalla presenza di bollicine
visibili o da un sibilo.
C. Se, dopo vari tentativi, l’esame di valutazione dell’integrità della cavità
non riesce, attenersi a quanto descritto nella sezione relativa alla
risoluzione dei problemi (punto 2.36) e interrompere la procedura.
Nota: se si rimuove il dispositivo monouso dalla cavità uterina
al termine dell’esame di valutazione, quando si reinserisce il
dispositivo sarà necessario rieseguire la prova prima di iniziare
l’ablazione (indipendentemente dall’esito dell’esame precedente).
2.37
Solo in modalità manuale
Quando si usa il sistema in modalità manuale, il ciclo di ablazione
non inizia automaticamente dopo il completamento con esito
positivo del test di valutazione dell’integrità della cavità. Dopo
aver completo con successo l’esame, premere il pulsante Attiva
e premere l’interruttore a pedale una seconda volta per avviare il
ciclo di ablazione.
Nota in alcuni controller RF modello 10, un controllo preliminare
del vuoto viene effettuato automaticamente prima dell’inizio del
ciclo di ablazione. Viene visualizzato il messaggio “Controllo
del vuoto in corso” e verrà emesso un segnale acustico per 10
secondi durante il controllo preliminare del vuoto.
Durante il ciclo di ablazione, viene visualizzata la schermata
“RFATTIVATA” con un timer che indica la durata dell’ablazione.
Nota: l’erogazione dell’energia in radiofrequenza può essere
interrotta in qualsiasi momento premendo l’interruttore a pedale.
2.38
Successivamente all’interruzione automatica del ciclo di ablazione
(che dura circa 90 secondi), ritrarre completamente il collare
cervicale nella posizione prossimale, premendo l’apposita linguetta.
Attenzione: il collare cervicale deve essere completamente retratto
in posizione prossimale al fine di ridurre al minimo la possibilità di
danni alla guaina quando si chiude l’array.
Collare
cervicale

17
ITALIANO
Una volta completato il ciclo di ablazione, sullo schermo viene
visualizzata la schermata “Procedura completata”, con un riepilogo
dei dati relativi alla procedura. La schermata “Procedura completata”
contiene, per ogni procedura, le informazioni seguenti:
• Lunghezza cavità
• Larghezza cavità
• Livello potenza
• Tempo di ablazione RF
2.39 Sbloccare il dispositivo monouso premendo il pulsante di rilascio.
Chiudere il dispositivo monouso tenendo fermo il perno anteriore e
tirare lentamente indietro le impugnature posteriori fino a quando
l’apposita spia, posizionata sui cardini delle impugnature anteriore
e posteriore, indica “ARRAY CHIUSO”. Questa indica che l’array è
stato retratto nella guaina del dispositivo monouso in posizione di
chiusura
Nota: in caso di difficoltà nel chiudere o rimuovere il dispositivo
monouso, consultare la sezione sulla risoluzione dei problemi,
“Problemi di chiusura e rimozione del dispositivo monouso nella
post-ablazione”.
Attenzione: per non danneggiare il dispositivo, retrarre l’array
con un movimento delicato.
2.40 Rimuovere il dispositivo monouso dalla paziente.
2.41 SPEGNERE IL CONTROLLER RF NOVASURE.
2.42 Eseguire le operazioni postoperatorie standard.
2.43 Dimettere la paziente dall’ospedale o dall’ambulatorio secondo le
indicazioni del medico curante.
Manutenzione periodica e assistenza
Il controller RF è stato progettato e testato nel rispetto della norma
IEC 60601–1 e di altri standard di sicurezza. La manutenzione
non è necessaria in quanto il sistema esegue degli autocontrolli
all’accensione. Per la pulizia del controller vedere la sezione “Pulizia e
sanificazione”.
La durata prevista dell’RFC è di cinque anni o 2.000 procedure a
condizione che si evitino danni da urto quali cadute o forti sollecitazioni.
Se il controller viene fatto cadere o subisce gravi urti, interrompere l’uso
e contattare l’assistenza tecnica Hologic. Fare riferimento alla sezione
“Assistenza tecnica e informazioni sulla restituzione del prodotto.
Il controller RF NovaSure non dispone di un manuale di manutenzione,
poiché l’unità non contiene alcun componente riparabile in loco.
Attenzione
: non sono consentite modifiche a questa apparecchiatura.
Test della potenza RF in uscita
Il controller RF NovaSure modello 10 incorpora l’esecuzione del test
della potenza RF in uscita nel test automatico eseguito all’avvio (test
POST). Durante il test POST, la potenza in uscita dal controller (Pc) viene
erogata in un resistore in parallelo (Rs) ubicato all’interno del controller.
La Pc desiderata è di 180 watt e l’Rs ha un valore nominale di 25
ohm. Durante il test POST non viene erogata potenza al connettore del
dispositivo monouso postosulla parte anteriore del controller.
Il controller RF NovaSure modello 10 esegue il test POST
automaticamente all’accensione. Per visualizzare le informazioni relative
al test POST, andare a Impostazioni, quindi scegliere Info. sistema.
Premere il pulsante “Info. versione”.
Nota: se ha luogo un errore di sistema durante il test POST, spegnere
e riaccendere l’alimentazione, quindi ripetere il test. Se si ripresenta
una condizione di errore di sistema, non usare il controller RF e
contattare l’assistenza clienti di Hologic.
Attenzione: non tentare di riparare il controller se si sospetta la
presenza di problemi. Attenersi alle indicazioni per la risoluzione di
problemi riportate nel presente manuale. Se il problema persiste,
chiamare l’assistenza tecnica Hologic per istruzioni.
Dispositivo monouso NovaSure sterile: non richiede alcuna manutenzione.
Da usarsi su una singola paziente. Non riusare e non risterilizzare il
dispositivo monouso NovaSure.
Icone dello schermo del controller RF NovaSure modello 10
Di seguito, è riportata la descrizione delle icone usate sullo schermo del
controller RF NovaSure modello 10.
Icona Impostazioni
Premere questo pulsante
per visualizzare le opzioni di
impostazione per la lingua, la
luminosità e il volume.
Icona Ultima procedura
Premere questo pulsante per
visualizzare la schermata
“Procedura completata” e
rivedere i dati di riepilogo relativi
all’ultima procedura effettuata.
Icona Guida
Premere questo pulsante per ottenere informazioni
addizionali sulla fase corrente della procedura.
L’iconavisualizza una versione ridotta della procedura
riportata nel documento delle istruzioni per l’uso.

18
ITALIANO
Nota: quando è premuta l’icona per l’ultima procedura, viene
visualizzata solo la procedura precedente. I dati relativi alle
procedure precedenti non saranno disponibili.
Nota: nella schermata “Impostazioni”, premere il pulsante “-” o
“+” per regolare il volume e la luminosità.
Nota: all’accendere per la prima volta il controller RF modello
10 viene visualizzata la schermata “Selezionare la lingua”.
L’impostazione predefinita è la lingua inglese. Per selezionare
una lingua diversa, premere il pulsante associato alla lingua
desiderata. Salvare la scelta effettuata premendo il pulsante verde
che lampeggia. La scelta della lingua viene così memorizzata. Per
modificare la lingua dopo l’impostazione iniziale, usare la schermata
“Impostazioni”. Per cambiare la lingua di visualizzazione delle
schermate, premere il nome della lingua di interesse. Per salvare
le modifiche apportate alle impostazioni, premere il pulsante verde
lampeggiante. Perannullare le selezioni effettuate, premere la “X”
blu.
Risoluzione delle condizioni di allarme più comuni
Allarme Dell’esame Cavità
Nel caso in cui l’esame non viene superato, viene visualizzato il messaggio
“Esame cavità non riuscito” unitamente alla versione ridotta della
procedura da seguire per risolvere il problema, riportata nella sua versione
integrale qui di seguito. L’esito negativo della valutazione dell’integrità
della cavità è dovuto all’impossibilità di pressurizzare la cavità. Le cause
possono essere le seguenti:
1. Perdita del dispositivo: verificare che sia stato installato il filtro
disidratante della linea di suzione. Controllare tutti i tubi e verificare
che siano stati serrati correttamente.
2. Perdita nell’orifizio esterno della cervice: verificare la presenza di
bollicine visibili o di un “sibilo” nell’orifizio esterno della cervice.
Premere la linguetta sul collare cervicale per far scivolare il collare
cervicale in avanti verso l’orifizio esterno della cervice in modo da
formare un sigillo a tenuta. Ripetere l’esame della valutazione della
cavità. Se anche questa volta l’esame non viene superato, usare
un secondo uncino per afferrare la cervice attorno alla guaina del
dispositivo monouso NovaSure. Ripetere l’esame della valutazione
della cavità.
3. Perforazione dell’utero: se si sospetta una perforazione, terminare
immediatamente la procedura.
Nota
: in presenza di una cervice eccessivamente dilatata, è possibile
che abbia luogo una perdita di CO2 in corrispondenza dell’orifizio
esterno del collo dell’utero. In queste condizioni la perdita di CO2 può
essere accompagnata dalla presenza di bollicine visibili o da un sibilo.
Nota: quando si segue la procedura per la risoluzione del problema
visualizzata sul controller RF modello 10, è possibile usare il
pulsante “?” e i pulsanti di scorrimento posti sulla destra per
ottenere maggiori informazioni. Per ritornare alla schermata
principale dopo la visualizzazione delle informazioni addizionali,
premere la “X” nell’angolo superiore destro dello schermo.
Se, dopo vari tentativi, l’esame di valutazione dell’integrità della cavità
non riesce, attenersi a quanto descritto nella sezione relativa alla
risoluzione dei problemi (punto 2.36) e interrompere la procedura.
Allarme del vuoto
La spia Vuoto si accende quando il livello del vuoto non rientra
nell’intervallo specificato. Tale condizione può essere causata da una o
più delle seguenti condizioni:
• cervice eccessivamente dilatata;
• scarso contatto tra il collare cervicale e l’orifizio esterno del collo
dell’utero;
• la valvola di sfiato del vuoto è bloccata in posizione chiusa;
• ostruzione nel disidratante oppure nel filtro o nei filtri (due) del
dispositivo monouso;
• ostruzione nel dispositivo monouso.
Se la prova del vuoto non riesce, sullo schermo viene visualizzato il
messaggio “Errore del vuoto” con una versione ridotta della procedura
dirisoluzione del problema, riportata integralmente qui di seguito:
• Premere delicatamente un dilatatore uterino o una sonda da
2–3,5 mm all’interno della valvola di sfiato del vuoto.
• Controllare la posizione del collare cervicale e, se necessario,
riposizionarla. Premere la linguetta sul collare cervicale per far
scivolare il collare cervicale in avanti verso l’orifizio esterno della
cervice in modo da formare un sigillo a tenuta. Verificare che non vi
sia una connessione allentata tra il collare cervicale e l’apertura del
canale cervicale che causi l’aspirazione di aria attraverso la cervice.
Nel caso in cui abbia luogo un’aspirazione di aria attraverso il canale
cervicale, provare a riposizionare il collare cervicale e lo stelo del
dispositivo monouso per prevenire l’ingresso di aria.
• Assicurarsi che il contenitore di suzione del dispositivo monouso sia
verticale e che la tubazione del dispositivo non tocchi la gamba della
paziente.
• Controllare tutti i tubi e verificare che siano stati serrati correttamente.
Controllare i connettori ad incastro dei tubi ubicati sul tubo del
disidratante. Se il disidratante è di colore rosa, sostituirlo. Assicurarsi
che il filtro posto vicino alla connessione monouso sulla linea del vuoto
sia ben saldo.
• Riprovare l’ablazione.
Se appare di nuovo il messaggio “Errore del vuoto”, procedere come segue:
• Disconnettere il dispositivo monouso dal controller RF.

19
ITALIANO
• Rimuovere il dispositivo monouso e sostituirlo con uno nuovo.
• Riprovare l’ablazione con il nuovo dispositivo.
Nota: quando si segue la procedura per la risoluzione del
problema visualizzata sul controller RF modello 10, è possibile
usare il pulsante “?” e i pulsanti di scorrimento posti sulla destra
per ottenere maggiori informazioni. Per ritornare alla schermata
principale dopo la visualizzazione delle informazioni addizionali,
premere la “X” nell’angolo superiore destro dello schermo.
Se si verifica un allarme del vuoto con il nuovo dispositivo, interrompere
la procedura.
Nota: se si rimuove il dispositivo monouso dalla cavità uterina
al termine dell’esame di valutazione, quando si reinserisce
il dispositivo sarà necessario rieseguire la prova prima di
iniziare l’ablazione (indipendentemente dall’esito dell’esame
precedente).
Contenitore CO2 quasi vuoto o vuoto
Viene visualizzata una schermata con il messaggio “Sostituire CO2” e
un’immagine della parte posteriore del controller. Viene emesso anche
un segnale acustico di un (1) bip al secondo. Gli eventuali messaggi di
allarme che erano già visibili prima che insorgesse questa condizione
di allarme rimangono invariati in presenza di un allarme dovuto a una
quantità insufficiente di CO2. La pressione dell’interruttore a pedale non
disattiverà il segnale acustico.
1. Sostituire il contenitore di CO2 per spegnere l’allarme.
Nota: non è necessario rimuovere il dispositivo monouso dalla
paziente prima di sostituire il contenitore.
2. Continuare con la procedura.
Allarme POSIZIONE ARRAY
Il messaggio “Posizione array” viene visualizzato quando l’array non è
aperto completamente. Il controller non è in grado di eseguire l’ablazione
in presenza di questo messaggio. Se ha luogo un allarme POSIZIONE
ARRAY, sullo schermo viene visualizzato il messaggio “Controllare
l’array” con una versione ridotta della procedura di risoluzione del
problema, riportata integralmente qui di seguito:
1. Spostare delicatamente l’estremità prossimale del dispositivo
monouso e notare se il messaggio “Posizione array” scompare.
Incaso contrario, procedere come indicato di seguito.
2. Con cura, provare a riposizionare il dispositivo monouso NovaSure:
A. Retrarre parzialmente l’array nella guaina, rilasciando il
pulsante di rilascio dell’impugnatura del dispositivo monouso.
B. Allontanare leggermente il dispositivo monouso dal fondo;
C. Lentamente, dispiegare di nuovo l’array del dispositivo monouso
spostando il dispositivo avanti e indietro con cura e bloccando le
impugnature; e
D. Riposizionare il dispositivo monouso contro il fondo attenendosi
alle istruzioni fornite nelle sezioni da 2.26 a 2.33.
3. Nel caso in cui la paziente abbia un utero retroverso, prestare particolare
attenzione per evitare una perforazione dello stesso. Mentre si posiziona
il dispositivo, applicare una leggera trazione caudale alla cervice usando
l’uncino ed alzare l’impugnatura del dispositivo verso l’alto (in linea con
l’asse dell’utero).
4. Se il messaggio “Posizione array” rimane visualizzato, retrarre
completamente l’array del dispositivo monouso e rimuovere il
dispositivo dalla paziente.
5. Dispiegare il dispositivo monouso esternamente alla paziente.
Assicurarsi che l’array di elettrodi non sia danneggiato e il
messaggio “Posizione array” scompaia.
6. Ritentare l’inserimento, il dispiegamento e il posizionamento del
dispositivo monouso attenendosi alla procedura descritta nella
sezione 2.0.
7. Se il messaggio “Posizione array” rimane visualizzato, sostituire il
dispositivo con uno nuovo.
8. Se il messaggio rimane visualizzato con un nuovo dispositivo
monouso, terminare la procedura.
Nota: quando si segue la procedura per la risoluzione del problema
visualizzata sul controller RF modello 10, è possibile usare il pulsante
“?” e i pulsanti di scorrimento posti sulla destra per ottenere
maggiori informazioni. Per ritornare alla schermata principale dopo
la visualizzazione delle informazioni addizionali, premere la “X”
nell’angolo superiore destro dello schermo.
Passare alla pagina successiva per la parte
rimanente delle Istruzioni per l’uso. Ulteriore
risoluzione dei problemi.

20
ITALIANO
Procedura non Completata
1. Rimuovere il dispositivo dalla paziente e dispiegare l’array
a. Verificare che l’array NON presenti danni
b. Verificare che NON appaia il messaggio relativo alla posizione dell’array
2. Per ulteriore assistenza premere il pulsante “?”
Una volta confermati i passaggi a e b, inserire nuovamente il dispositivo e
PREMERE L’INTERRUTTORE A PEDALE per ritentare il trattamento.
Se si riscontrano problemi, sostituire il dispositivo e riavviare la procedura.
1. Rimuovere il dispositivo monouso NovaSure dall’utero, dopo aver
retratto l’array nella guaina attenendosi alla seguente procedura.
A. Rilasciare il pulsante di rilascio del dispositivo monouso.
B. Mantenere ferma l’impugnatura frontale del dispositivo monouso.
C. Tirare l’impugnatura posteriore del dispositivo monouso.
2. Ispezionare il dispositivo monouso per rilevare eventuali danni.
Dispiegare completamente l’array di elettrodi esternamente alla
paziente, assicurandosi che il messaggio non venga visualizzato sul
dispositivo.
3. Se il dispositivo monouso non è danneggiato e il messaggio su
schermo non viene visualizzato sull’RFC modello 10, inserire e
dispiegare nuovamente il dispositivo, quindi ritentare il trattamento.
4. Se il problema persiste, sostituire il dispositivo monouso con uno
nuovo.
5. Riprovare a eseguire la procedura. Se il problema persiste, terminare
la procedura.
La schermata “RF ON” (RF ATTIVATA) non verrà visualizzata
sull’RFC modello 10.
1. Nel caso in cui il controller RF NovaSure è collegato all’alimentazione
e acceso e il pulsante Attiva è stato premuto, ma non viene erogata
potenza dal controller alla pressione dell’interruttore a pedale,
controllare i collegamenti con l’interruttore a pedale. Verificare inoltre
che l’esame DELLA CAVITÀ SIA COMPLETATO E RIUSCITO.
2. Se il problema persiste, terminare la procedura.
I valori SU/GIÙ non vengono visualizzati quando si premono
itasti corrispondenti
Assicurarsi che il dispositivo monouso sia collegato al controller.
Ivalori sono visualizzati solo nel caso in cui il dispositivo monouso sia
correttamente collegato al controller.
Istruzioni per la sostituzione di componenti
Il controller RF NovaSure utilizza un paio di fusibili che sono collocati
su un portafusibili nel modulo di entrata dell’alimentazione. Si tratta di
fusibili del tipo T5AH, 250 V. Per accedere al modulo, usare un cacciavite
a stella per aprire lo sportellino del portafusibili. Se necessario, è
possibile rimuovere il portafusibili per sostituire i fusibili. Per rimontare
il portafusibili, seguire la procedura inversa. Eventuali prodotti NovaSure
difettosi devono essere restituiti a Hologic per essere ispezionati.
Attenersi alle istruzioni riportate alla fine del presente manuale, nella
Possibile perforazione dell’utero
Prima dell’erogazione di energia:
1. Terminare la procedura.
2. Verificare la stabilità della
paziente.
3. Valutare la necessità di
eseguire gli esami necessari
a rilevare una eventuale
perforazione.
4. Riprogrammare la procedura,
se necessario.
Durante o dopo l’erogazione di
energia:
1. Terminare la procedura.
2. Verificare la stabilità della
paziente.
3. Verificare che non vi siano
lesioni alle viscere.
4. Riprogrammare la procedura,
se necessario.
L’array non si dispiega completamente per bloccarsi nell’utero
1. Rimuovere parzialmente l’array nella guaina (mantenere ferma
l’impugnatura frontale e tirare quella posteriore allontanandola dalla
paziente).
2. Riposizionare il dispositivo monouso nella cavità.
3. Dispiegare nuovamente l’array nella cavità.
4. Se il dispositivo monouso non si blocca, rimuoverlo dall’utero.
5. Ispezionare il dispositivo monouso per rilevare eventuali danni.
6. Provare ad aprire e bloccare il dispositivo monouso esternamente alla
paziente.
7. In presenza di danni, sostituire il dispositivo monouso.
8. Se il dispositivo monouso non è danneggiato, reinserirlo nella cavità
uterina della paziente e dispiegarlo.
9. Se risulta impossibile dispiegare il dispositivo monouso a una
distanza tra corni di almeno 2,5 cm, terminare la procedura.
10. Valutare la possibilità che il mancato dispiegamento sia dovuto a una
perforazione dell’utero.
Problemi di chiusura e rimozione del dispositivo monouso nella
post-ablazione
Confermare che il pulsante di rilascio del blocco è premuto:
• In tal caso, retrarre gradualmente il dispositivo monouso dalla
paziente.
• In caso contrario, premere il pulsante di rilascio del blocco e tentare
nuovamente di chiudere il dispositivo monouso. Se la chiusura risulta
ancora difficile, retrarre gradualmente il dispositivo monouso dalla
paziente.
La schermata “Procedure complete” (Procedura completata)
non viene visualizzata sull’RFC modello 10 al termine di una
procedura.
Se il dispositivo non è stato collegato all’alimentazione per almeno 30
secondi, la schermata “Procedure complete” (Procedura completata)
non verrà visualizzata sull’RFC modello 10. Rimuovere il dispositivo
monouso NovaSure dall’utero, dopo aver retratto l’array nella guaina
attenendosi alla seguente procedura.

21
ITALIANO
sezione Restituzioni, per ottenere un numero di autorizzazione al reso
(num. RMA). Non gettare il dispositivo monouso NovaSure.
Specifiche tecniche
Dispositivo monouso NovaSure
1. Il dispositivo monouso NovaSure non contiene lattice.
2. Sulla base delle normative della FDA, il dispositivo monouso
NovaSure è un dispositivo di classe III.
3. Il dispositivo monouso NovaSure è un dispositivo di classe IIb,
secondo quanto stabilito dalla Normativa MDD 93/42/CEE.
4. Il diametro nominale della punta del dispositivo monouso NovaSure
è6 mm.
5. Le dimensioni del dispositivo monouso NovaSure sono le seguenti:
48,3 x 15,2 x 5 cm (19" x 6" x 12").
6. Il dispositivo monouso NovaSure ha una tensione nominale di 153 Volt.
Controller RF NovaSure
1. Il controller RF NovaSure può essere utilizzato con uscite che
forniscono da 100 a 240 V c.a. e assorbe un massimo di 5 A.
2. Il controller RF NovaSure è un dispositivo di classe I del tipo BF,
conformemente a quanto stabilito dalla normativa CEI 60601-1.
3. Sulla base delle normative della FDA, il controller RF NovaSure è un
dispositivo di classe III.
4. Il controller RF NovaSure è un dispositivo di classe IIB, secondo
quanto stabilito dalla Normativa MDD 93/42/CEE.
5.
Il controller RF è stato testato ed è risultato essere conforme ai
limiti per i dispositivi medici previsti dalla norma IEC 60601–1–2
ED 4.0: 2014.
Tali limiti sono stati stabiliti per garantire una protezione
adeguata contro ogni interferenza nociva in un tipico ambiente di tipo
ospedaliero. Questa apparecchiatura genera, utilizza e può irradiare
energia di radiofrequenza e, qualora non fosse installata conformemente
alle istruzioni, potrebbe causare un’interferenza dannosa ad altri
dispositivi collocati nelle vicinanze. Non esiste tuttavia alcuna garanzia
che l’interferenza non si verifichi in una particolare installazione.
Qualora l’apparecchiatura causasse un’interferenza dannosa ad altri
dispositivi, ilche può essere determinato accendendo e spegnendo
l’apparecchiatura, si consiglia di provare a correggere l’interferenza in
uno dei seguenti modi:
• Cambiare l’orientamento o la posizione dei dispositivi.
• Aumentare la distanza tra i dispositivi.
• Collegare lo strumento a una presa che faccia parte di un circuito
diverso rispetto a quello cui sono collegati gli altri dispositivi.
• Per assistenza, contattare il servizio tecnico Hologic (o il produttore
dell’altra apparecchiatura).
6. Il controller è conforme ai requisiti stabiliti dalle normative
CEI60601-1/UL60601-1, CEI60601-2-2 e CSAC22.2No. 601.1.
7. La spedizione del controller deve avvenire esclusivamente nel
contenitore originale usato da Hologic. Di seguito sono indicate
le specifiche ambientali per il funzionamento, la spedizione e la
conservazione.
8. Il picco di tensione assoluta massima generato dal controller
RFNovaSure è di 153 Volt. Gli accessori utilizzati con il controller
RFdevono avere una tensione nominale pari o superiore a 153 Volt.
9. Il picco di tensione assoluta massima generato dal controller
RFNovaSure è di 216 watt.
10. Peso del controller RF NovaSure: 11kg, senza confezione.
11. Altezza: 32 cm; larghezza: 19 cm; profondità: 35,5 cm.
(12,5" x 7,5" x 14,5")
12. La pressione massima di CO2 erogata dal controller RF NovaSure e dal
dispositivo monouso deve essere di 90 ±10mmHg. Il flusso massimo
di CO2 del controller RF NovaSure con un dispositivo monouso
collegato è di 95 ±15ml/min (il flusso massimo di CO2 del controller
RF NovaSuresenza dispositivo monouso collegato è di 105 - 130ml/
min).
13. Il generatore RF NovaSure deve essere utilizzato senza elettrodo
neutro.
Potenza vs. resistenza
Potenza misurata (watt)
Resistenza di carico (ohm)
Potenza effettiva vs. impostazione di potenza in un carico di 20 ohm
Potenza effettiva (watt)
Impostazione di potenza (watt)

22
ITALIANO
Informazioni sulla sicurezza elettromagnetica
Tabella 1 - Guida e dichiarazione del produttore – Emissioni
elettromagnetiche
Linee guida e dichiarazione del produttore - Emissioni
elettromagnetiche
Il controller RF NovaSure è prodotto per l’uso nell’ambiente
elettromagnetico specificato di seguito. Il cliente o utente del
controller RF NovaSure deve accertarsi che il prodotto venga
utilizzato in questo tipo di ambiente.
Test delle
emissioni Conformità Ambiente elettromagnetico – Guida
Emissioni RF
CISPR 11
Gruppo 1 Per poter svolgere la funzione per
la quale è progettato, il controller
RF NovaSure deve emettere energia
elettromagnetica. Le attrezzature
elettroniche nelle vicinanze potrebbero
risentirne.
Emissioni RF
CISPR 11
Classe A Il controller RF NovaSure è destinato
all’uso in strutture sanitarie
professionali come ospedali e studi
medici.
Avvertenza: le caratteristiche in
termini di EMISSIONI di questa
apparecchiatura la rendono
idonea all’uso in aree industriali e
ospedaliere (CISPR 11 classe A).Se
utilizzata in ambiente residenziale
(per il quale è normalmente
richiesto il rispetto della norma
CISPR 11 classe B), questa
apparecchiatura potrebbe non
offrire una protezione adeguata
ai servizi di comunicazione
a radiofrequenza.L’utente
potrebbe dover adottare
misure di mitigazione, come il
riposizionamento o il riorientamento
dell’apparecchiatura.
Emissioni
armoniche
IEC 61000-
3-2
Classe A
Fluttuazioni
di tensione/
emissioni
flicker IEC
61000–3–3
Conforme
Avvertenza: in alcune circostanze, sussiste il rischio di ustioni in
siti alternativi, quando si utilizza un dispositivo ad alta frequenza.
Si deve evitare il contatto pelle a pelle, per esempio con
l’inserimento di una garza asciutta.
Avvertenza: con qualsiasi dispositivo elettroshock esiste il
rischio di formazione di archi e può verificarsi stimolazione
neuromuscolare. Se il dispositivo viene utilizzato correttamente
nell’utero, il rischio di stimolazione muscolare, in particolare al
muscolo cardiaco, è remoto.
Condizioni ambientali
Controller RF NovaSure
Condizioni di funzionamento senza confezione
Altitudine da 0 a 3.030 m (da 0 a 10.000 piedi)
Temperatura da 10 °C a 40 °C (da 50 °F a 104 °F)
Umidità dal 15 all’85% di umidità relativa
(senzacondensa)
Condizioni di inattività nella confezione
Altitudine da 0 a 12.120 m (da 0 a 40.000 piedi)
Temperatura da -30 °C a 60 °C (da -22 °F a 140 °F)
Umidità 85% di umidità relativa, (senzacondensa)
fino al 90% di umidità relativa (senza condensa)
Caratteristiche importantisul funzionamento
• Prima dell’inserimento del dispositivo nel paziente, l’aria deve essere
espulsa dal dispositivo per 10 secondi.
• Affinché la valutazione dell’integrità della cavità (CIA) abbia esito
positivo, la pressione misurata deve essere pari a 50 ± 10 mmHg per
almeno 3 secondi. In caso contrario, la valutazione CIA segnalerà un
errore.Il controller RF non abilita l’ablazione fino a quando il test CIA
non ha esito positivo.
• Potenza RF: l’intervallo di potenza RF è compresa tra 55 e 180 (+/-
20%) watt.
• Monitoraggio della pressione di vuoto: durante un’ablazione la
pressione di vuoto deve essere compresa tra 17,78 ± 5,1 mmHg e
152,4 ± 25,4 mmHg.Se la pressione di vuoto supera questo intervallo,
il controller terminerà l’ablazione.
• Monitoraggio dell’impedenza: il controller RF interrompe un’ablazione
quando l’impedenza del tessuto misurata raggiunge all’incirca i
50 ohm.
• Timer di due minuti: dopo due minuti di erogazione di energia RF, il
controller terminerà l’ablazione.
• Timeout di dieci minuti: dopo aver completato la procedura di
ablazione il controller si disattiva per 10 minuti; in questo periodo il
controller non è in grado di erogare energia.
• Protezione da cortocircuito c.c.: se il controller RF rileva un
cortocircuito (cioè un valore < 13 +/- 6 ohm), l’ablazione verrà
interrotta.

23
ITALIANO
Tabella 2 - Linee guida e dichiarazione del produttore -
Immunità elettromagnetica
Guida e dichiarazione del produttore – Immunità
elettromagnetiche
lI controller RF NovaSure è prodotto per l’uso nell’ambiente
elettromagnetico specificato di seguito. Il cliente o utente del
controller RF NovaSure deve accertarsi che il prodotto venga
utilizzato in questo tipo di ambiente.
Test di
immunità Livello di test
IEC 60601 Conformità
Livello
Ambiente
elettromagnetico –
Guida
Scariche
elettrostatiche
(ESD)
IEC 61000-
4-2
Contatto ±2 kV,
±4 kV, ±8 kV
Contatto ±2 kV,
±4 kV, ±8 kV
I pavimenti devono
essere in legno,
cemento o mattoni
di ceramica.
Se i pavimenti
sono rivestiti con
materiale sintetico,
l’umidità relativa
deve essere almeno
del 30%.
Aria ±2 kV,
±4 kV, ±8 kV,
±15 kV
Aria ±2 kV,
±4 kV, ±8 kV,
±15 kV
Transitori
elettrici
veloci/burst
IEC 61000-
4-4
±0,5 kV,
±1 kV, ±2 kV
per le linee di
alimentazione
elettrica
Frequenza
di ripetizione
100 kHz
±0,5 kV,
±1 kV, ±2 kV
per le linee di
alimentazione
elettrica
Frequenza
di ripetizione
100 kHz
La qualità
dell’alimentazione
di rete deve essere
quella di un tipico
ambiente ospedaliero
o commerciale.
Sovratensione
IEC 61000-
4-5
±0,5 kV, ±1 kV
da linea a linea
±0,5 kV, ±1 kV
da linea a linea
La qualità
dell’alimentazione
di rete deve essere
quella di un tipico
ambiente ospedaliero
o commerciale.
±0,5 kV, ±1 kV,
±2 kV da linea
a terra
±0,5 kV, ±1 kV,
±2 kV da linea
a terra
Cali di
tensione,
brevi
interruzioni
e variazioni
di tensione
sulle linee di
alimentazione
elettrica in
ingresso
IEC 61000-
4-11
0% UT; 0,5 ciclo
a 0°, 45°, 90°,
135°, 180°,
225°, 270° e
315°
0% UT; 0,5 ciclo
a 0°, 45°, 90°,
135°, 180°,
225°, 270° e
315°
La qualità
dell’alimentazione
di rete deve essere
quella di un tipico
ambiente ospedaliero
o commerciale. Se
l’utente del controller
RF NovaSure richiede
il funzionamento
continuo durante le
interruzioni della rete
di alimentazione,
si consiglia di
alimentare il
controller mediante
una batteria
o una fonte di
alimentazione
continua.
0% UT; 1 ciclo e
70% UT;
25/30 cicli
Monofase: a 0°
0% UT; 1 ciclo e
70% UT;
25/30 cicli
Monofase: a 0°
0% UT; 250 cicli 0% UT; 250 cicli
Questa
condizione fa sì
che il controller
RF si spenga
e poi ritorni
in modalità
standby.
Frequenza di
rete 50/60Hz
Campo
magnetico
IEC 61000-
4-8
30 A/m
50 Hz
30 A/m
50 Hz
I campi magnetici
di frequenza della
potenza devono
essere quelli di un
tipico ambiente
ospedaliero
o commerciale.
Nota: Ut è la tensione di rete prima che vengano applicati i livelli
di test.

24
ITALIANO
Tabella 3 - Guida e dichiarazione del produttore – Emissioni
elettromagnetiche
Guida e dichiarazione del produttore – Emissioni
elettromagnetiche
I controller RF NovaSure è prodotto per l’uso nell’ambiente
elettromagnetico specificato di seguito. Il cliente o utente del controller
RF NovaSure deve accertarsi che il prodotto venga utilizzato in questo
tipo di ambiente.
RF condotta
IEC 61000-
4-6
3 V
0,15 MHz -
80 MHz
6 V in ISM e
le bande radio
amatoriali tra
0,15 MHz e
80 MHz
80% AM a
1 kHz
3 V
0,15 MHz -
80 MHz
6 V in ISM
e le bande
radio
amatoriali tra
0,15 MHz e
80 MHz
80% AM a
1 kHz
RF irradiata
IEC 61000-
4-3
3 V/m
Da 80 MHz a
2,7 GHz
80% AM a
1 kHz
3 V/m
Da 80 MHz a
2,7 GHz
80% AM a
1 kHz
Distanza di separazione minima
raccomandata
Le apparecchiature di comuni-
cazione RF portatili (comprese le
periferiche come i cavi d’antenna
e le antenne esterne) devono
essere utilizzate ad almeno
30cm (12pollici) di distanza
da qualsiasi parte del sistema
di ablazione endometriale a
impedenza NovaSure, compresi
i cavi specificati da Hologic Inc.
In caso contrario, le prestazioni
dell’apparecchiatura potrebbero
venire compromesse.
L’intensità di campo dai
trasmettitori di radiofrequenza
fissi, stabilita con un’indagine sul
sito elettromagnetico,a deve essere
inferiore al livello di conformità in
ciascun intervallo di frequenza.b
Possono verificarsi interferenze in
prossimità di apparecchiature che
riportano il seguente simbolo:
NOTA 1: a 80 MHz e 800 MHz, si applica l’intervallo di frequenza maggiore.
NOTA 2: queste linee guida potrebbero non essere applicabili per tutte le
situazioni. La propagazione elettromagnetica è influenzata dall’assorbimento e
dal riflesso di strutture, oggetti e persone.
a
Le intensità di campo prodotte da trasmettitori fissi, quali le stazioni base per telefoni a radiofrequenza (cellulari/
cordless) e radiomobili, radioamatoriali, trasmissioni radiofoniche AM e FM e trasmissioni TV non possono essere
valutate con precisione. Per valutare l’ambiente elettromagnetico in relazione ai trasmettitori di radiofrequenza fissi,
occorre considerare di effettuare un’indagine sul sito elettromagnetico. Se l’intensità di campo misurata nel luogo in
cui il generatore di radiofrequenza viene utilizzato supera il livello di conformità di radiofrequenza applicabile indicato,
occorre controllare il generatore per verificarne il normale funzionamento. Se si riscontra un funzionamento anomalo,
potrebbero essere necessarie delle misure aggiuntive, quali il riorientamento o il ricollocamento del generatore di
radiofrequenza.
b
Oltre l’intervallo di frequenza da 150 kHz a 80 MHz, le intensità di campo devono essere inferiori a 3 V/m.
Distanze di separazione raccomandate tra le apparecchiature
per comunicazioni in radiofrequenza portatili e mobili e il
controller RF NovaSure
Le apparecchiature di comunicazione RF portatili (comprese le
periferiche come i cavi d’antenna e le antenne esterne) devono essere
utilizzate ad almeno 30cm (12pollici) di distanza da qualsiasi parte del
sistema di ablazione endometriale a impedenza NovaSure, compresi
i cavi specificati da Hologic Inc. In caso contrario, le prestazioni
dell’apparecchiatura potrebbero venire compromesse.
Pulizia e disinfezione
Si raccomanda l’uso di agenti non infiammabili per la pulizia e la
disinfezione. Gli agenti o solventi infiammabili per la pulizia e la disinfezione
devono essere fatti evaporare prima di essere usati per il sistema NovaSure.
Il controller RF NovaSure non è sterile. Pulire le superfici con una
soluzione di acqua e detergente delicato. Non immergere l’unità in liquidi
e non introdurre liquidi nelle ventole di raffreddamento o nelle aree
contenenti cavi in radiofrequenza.
Il dispositivo monouso NovaSure è un dispositivo sterile da utilizzarsi su
una singola paziente.
• Non usare se la confezione è aperta o danneggiata.
• Non riusare e non risterilizzare il dispositivo monouso.
Non sterilizzare alcun componente del sistema di ablazione endometriale
NovaSure a impedenza.

25
ITALIANO
Lista delle parti
Informazioni per gli ordini/parti e accessori
Codice prodotto Descrizione
RFC2010 Controller RF NovaSure, modello 10
814002 Cavo di alimentazione, 115 Volt, Nord America
814003 Cavo di alimentazione, 230 Volt, Europa
814004 Cavo di alimentazione, 220 Volt, Regno Unito/
Irlanda
814005 Cavo di alimentazione, Danimarca
814009 Cavo di alimentazione, Italia
814011 Cavo di alimentazione, Svizzera
814015 Cavo di alimentazione, Giappone
814016 Cavo di alimentazione, Australia
52124-001 Interruttore a pedale
815012 CO2 (USP), bombola, 5 unità
NS2013 Kit dispositivo monouso per sistema di ablazione
endometriale NovaSure a impedenza
300001 Kit per prodotti a rischio biologico
Smaltimento
ATTENZIONE: Il dispositivo monouso va trattato come rifiuto a
rischio biologico e deve pertanto essere smaltito in conformità
alle normative vigenti nell’istituto per i rifiuti di questo tipo.
Hologic, i distributori e i clienti della Comunità Europea devono
soddisfare la Direttiva sullo smaltimento delle apparecchiature
elettriche ed elettroniche (WEEE) (2002/96/EC). Hologic si impegna
a soddisfare i requisiti specifici dei vari paesi affinché i suoi prodotti
rispettino e tutelino l’ambiente. L’obiettivo di Hologic è ridurre i rifiuti
derivanti dallo smaltimento dei suoi dispositivi elettrici ed elettronici.
Hologic mette in pratica i vantaggi derivanti dal rispetto della direttiva
WEEE per un potenziale riutilizzo, trattamento, riciclo o recupero, volti
a ridurre al minimo la quantità di sostanze pericolose che vengono
immesse nell’ambiente. I clienti Hologic della Comunità Europea hanno
la responsabilità di garantire che i dispositivi medici contrassegnati dal
seguente simbolo, che indica l’applicazione della direttiva WEEE, non
siano smaltiti nei rifiuti urbani se non espressamente autorizzato dalle
autorità locali.
Contattare l’assistenza tecnica Hologic per organizzare uno smaltimento
adeguato del controller RF conformemente alla Direttiva WEEE.
Garanzia
Salvo quanto diversamente ed espressamente indicato nel contratto: i)
Si garantisce al cliente originario che le prestazioni dell’apparecchiatura
prodotta da Hologic rimarranno sostanzialmente conformi alle
specifiche del prodotto pubblicate per il periodo di un (1) anno a partire
dalla data di spedizione o, se è richiesta l’installazione, dalla data di
installazione (“Periodo di garanzia”); ii) i tubi radiogeni per imaging
mammografico digitale sono garantiti per ventiquattro (24) mesi,
durante i quali i tubi sono completamente coperti da garanzia per
i primi dodici (12) mesi e sono garantiti secondo il metodo lineare
prorata temporis durante i mesi 13-24; iii) i pezzi di ricambio e gli
elementi rigenerati sono garantiti per la durata rimanente del periodo
di garanzia o per novanta (90) giorni dalla spedizione, a seconda
del periodo superiore; iv) si garantisce che i materiali di consumo
rimarranno conformi alle specifiche pubblicate per un periodo che
termina alla data di scadenza indicata sulle rispettive confezioni; v)
si garantisce che il funzionamento rimarrà conforme alle specifiche
pubblicate; vi) si garantisce che i servizi saranno prestati a regola
d’arte; vii) le apparecchiature che non sono prodotte da Hologic sono
garantite tramite il proprio produttore e tali garanzie si estendono
ai clienti Hologic nella misura concessa dal produttore di tali
apparecchiature non prodotte da Hologic. Hologic non garantisce che
l’utilizzo di tali prodotti sarà ininterrotto o esente da errori, né che i
prodotti possano funzionare con prodotti di terzi non autorizzati da
Hologic.
Le presenti garanzie non si applicano a nessun articolo: che venga (a)
riparato, spostato o alterato da personale di servizio non autorizzato
da Hologic; che sia (b) sottoposto ad abuso, utilizzo eccessivo o uso
improprio (compresi termico o elettrico); che venga (c) conservato,
riparato o azionato in modo incompatibile con le specifiche o le
istruzioni di Hologic applicabili, compreso il rifiuto da parte del Cliente di
acconsentire agli aggiornamenti del Software raccomandati da Hologic;
oppure che sia (d) designato come soggetto a una garanzia non Hologic
o pre-release o secondo il principio “così com’è”.
Assistenza tecnica e informazioni per la restituzione dei
prodotti
Avvertenza: se si fa cadere il controller RF la garanzia viene
automaticamente annullata. Una caduta può danneggiare il
controller in modo tale da renderlo non riparabile. Si raccomanda di
usare un carrello stabile dotato di dispositivi di fissaggio per ridurre
il rischio che il controller cada. Prestare particolare attenzione
durante il trasporto del controller RF a un’altra sede. Per qualsiasi
domanda sul controller RF, chiamare il numero 1-800-442-9892 o
(508) 263-2900.

26
ITALIANO
Glossario dei simboli
Simbolo Riferimento
standard e
numero simbolo
Denominazione
simbolo Descrizione simbolo
EC R
EP EN ISO 15223-1,
5.1.2
Rappresentante
autorizzato
nella Comunità
Europea
Indica il
rappresentante
autorizzato nella
Comunità Europea.
IEC 60601-1,
Tabella D.1, 1
IEC 60417, 5032
Corrente alter-
nata (c.a.)
Indica sulla targhetta
che l’apparecchiatura
è idonea
esclusivamente per
la corrente alternata;
identifica i terminali
pertinenti.
EN ISO 15223-1,
5.3.9
ISO 7000, 2621
Limite di pressio-
ne atmosferica
Indica i valori limite
della pressione
atmosferica alla quale
il dispositivo medico
può essere esposto in
modo sicuro.
EN ISO 15223-1,
5.1.5
ISO 7000, 2492
Codice lotto
Indica il codice del
lotto del produttore
per l’identificazione
della partita o del lotto
stesso.
CO2N/A Diossido di
carbonio Indica la presenza di
anidride carbonica.
EN ISO 15223-1,
5.1.6
ISO 7000, 2493
Numero di ca-
talogo
Indica il numero di
catalogo del produttore
per l’identificazione del
dispositivo medico.
N/A Categoria ap-
parecchiatura
non AP
Identifica le
apparecchiature di
categoria non AP.
EN ISO 15223-1,
5.4.4
ISO 7000, 0434A
IEC 60601-1,
Tabella D.1, 10
Attenzione
Indica che occorre fare
attenzione quando si
azionano i comandi
o il dispositivo in
prossimità del punto
in cui è posizionato il
simbolo, oppure indica
che la situazione
operativa richiede
la consapevolezza
dell’operatore o
un’azione da parte
dell’operatore per
evitare conseguenze
indesiderate.
Centri di assistenza
Nel caso in cui il controller RF NovaSure cessasse di funzionare,
contattare l’assistenza tecnica di Hologic per le istruzioni e per ottenere
un numero di autorizzazione al reso (NUM. RMA). Pulire e confezionare
il controller in modo adeguato e restituirlo per la riparazione a uno dei
centri autorizzati elencati di seguito. Se il controller non è in garanzia,
verranno addebitati i costi per la riparazione, determinabili a seguito
della ricezione e dell’ispezione del controller in questione.
Per maggiori informazioni
Per supporto tecnico o informazioni sulla riordinazione negli Stati Uniti,
contattare:
Hologic, Inc.
250 Campus Drive
Marlborough, MA 01752 USA
Tel.: 800-442-9892 (numero verde)
www.hologic.com
Nota: qualsiasi evento ritenuto un problema di sicurezza va riferito
al dipartimento di assistenza tecnica Hologic.
I clienti internazionali devono contattare il distributore o il rappresentante
Hologic di zona:
Hologic BV
Da Vincilaan 5
1930 Zaventem
Belgium
Tel: +32 2 711 46 80
Fax: +32 2 725 20 87
Inoltrare a Hologic qualsiasi reclamo o problema relativi a qualità,
affidabilità, sicurezza o prestazioni di questo prodotto. Se il dispositivo ha
causato nuove o altre lesioni alla paziente, segnalare immediatamente
l’accaduto al rappresentante autorizzato Hologic e all’autorità
competente del proprio Stato membro o Paese. Le autorità competenti in
materia di dispositivi medici sono generalmente il ministero della Salute
dei singoli Stati membri o un’agenzia all’interno del Ministero della
Salute.
Contattare l’assistenza tecnica Hologic se il dispositivo monouso
NovaSure o il controller RF non funziona come previsto. Se il prodotto
deve essere restituito a Hologic per qualunque motivo, l’assistenza
tecnica fornirà un numero di autorizzazione al reso (RMA) ed
eventualmente il kit per prodotti a rischio biologico.
Restituire i controller RF secondo le istruzioni fornite dall’assistenza
tecnica. Pulire il controller RF prima di restituirlo e inserire tutti gli
accessori nella confezione con l’unità restituita.
Restituire dispositivi monouso usati o aperti secondo le istruzioni fornite
con il kit per prodotti a rischio biologico di Hologic.

27
ITALIANO
Simbolo Riferimento
standard e
numero simbolo
Denominazione
simbolo Descrizione simbolo
Direttiva europea
sui dispositivi
medici 93/42/
CEE, Articolo 17 e
Allegato XII
Regolamento
europeo sui
dispositivi medici
2017/745,
Allegato V
Marchio CE
di conformità
con numero di
identificazione
dell’organismo
notificato
Indica che il dispositivo
medico è conforme
alla Direttiva europea
sui dispositivi medici
93/42/CEE e soddisfa
i requisiti applicabili
in materia di salute,
sicurezza e ambiente.
Se il simbolo è
accompagnato da un
numero significa che la
conformità è verificata
dall’ente notificato
indicato.
EN ISO 15223-1,
5.4.3
ISO 7000, 1641
IEC 60601-1,
Tabella D.1, 11
Consultare le
Istruzioni per
l’uso
Indica la necessità per
l’utente di consultare
le istruzioni per l’uso.
CC
ISO/DIS 15223-1,
5.7.11
ISO 7000, 6049
Paese di produzi-
one
Identifica il Paese
di produzione dei
prodotti.
IEC 60601-1,
Tabella D.1, 24
IEC 60417, 5036
Tensione peri-
colosa
Indica i pericoli
derivanti da tensioni
pericolose.
EN ISO 15223-1,
5.1.3
ISO 7000, 2497
Data di fabbrica-
zione
Indica la data in cui il
dispositivo medico è
stato prodotto.
IEC 60601-1,
Tabella D.1, 26
IEC 60417, 5334
Apparecchiatura
tipo BF a prova di
defibrillatore
Identifica un
componente di
tipo BF a prova
di defibrillazione
conforme alla norma
IEC 60601-1.
EN ISO 15223-1,
5.2.6
ISO 7000, 2608
Non
risterilizzare
Indica che il dispositivo
medico non deve
essere risterilizzato.
EN ISO 15223-1,
5.4.2
ISO 7000, 1051
IEC 60601-1,
Tabella D.1, 28
Non riutilizzare
Indica che il
dispositivo medico
è esclusivamente
monoso.
ISO 7000, 2403
ISO 780
Non accatastare
più di “n”
Indica che gli
articoli non devono
essere impilati
verticalmente oltre il
numero specificato,
a causa della natura
dell’imballaggio di
trasporto o degli
articoli stessi.
Simbolo Riferimento
standard e
numero simbolo
Denominazione
simbolo Descrizione simbolo
EN ISO 15223-1,
5.2.8
ISO 7000, 2606
Non usare se
la confezione è
danneggiata
Indica che il dispositivo
medico non deve
essere utilizzato se
la confezione è stata
danneggiata o aperta
e che l’utente deve
consultare le istruzioni
per l’uso per ottenere
ulteriori informazioni.
IEC 60601-1,
Tabella D.1, 8
IEC 60417, 5021
Massa equipo-
tenziale
Identifica i terminali
che, quando collegati
tra loro, portano
i componenti di
un’apparecchiatura
o di un sistema allo
stesso potenziale,
non necessariamente
il potenziale di terra,
ad esempio per il
collegamento locale.
Direttiva WEEE
2002/96/EC
2012/19/EC
EN 60417, 6414
Direttiva della
Comunità Euro-
pea sullo smalti-
mento delle
apparecchia-
ture elettriche
ed elettroniche
(WEEE) 2002/96/
EC
Indica la necessità
di smaltire
separatamente le
apparecchiature
elettriche ed
elettroniche (RAEE).
ISO 7010
ISO 3864-2,
M002
Seguire le istru-
zioni per l’uso
Indica la necessità di
leggere il manuale/
libretto di istruzioni.
IEC 60417, 5114 Interruttore a
pedale
Indica la presenza
di un interruttore
a pedale o la
connessione per un
interruttore a pedale.
EN ISO 15223-1,
5.3.1
ISO 7000, 0621
ISO 780
Fragile
Indica che il dispositivo
medico che può essere
rotto o danneggiato se
non viene manipolato
con cura.
IEC 60143-1,
5016 Limiti di umidità Indica la presenza di
scatole dei fusibili o la
loro posizione.
HP N/A Alta pressione IIndica la presenza di
alta pressione.
EN ISO 15223-1,
5.3.8
ISO 7000, 2620
Limiti di umidità
Indica i valori limite
di umidità ai quali il
dispositivo medico
può essere esposto in
modo sicuro.

28
ITALIANO
AW-22724-701 Rev. 001
04/2022
Simbolo Riferimento
standard e
numero simbolo
Denominazione
simbolo Descrizione simbolo
EN ISO 15223-1,
5.3.2
ISO 7000, 0624
ISO 780
Proteggere dal
calore
Indica la necessità
di proteggere il
dispositivo medico da
fonti di calore.
EN ISO 15223-1,
5.3.4
ISO 7000, 0626
ISO 780
Mantenere
asciutto
Indica la necessità
di proteggere il
dispositivo medico
dall’umidità.
EN ISO 15223-1,
5.1.1
ISO 7000, 3082
Fabbricante Indica il produttore del
dispositivo medico.
ISO/DIS 15223-1,
5.7.7 Dispositivo
medico Indica che l’articolo è
un dispositivo medico.
N/A Niente olio Indica l’assenza di olio.
EN ISO 15223-1,
5.1.7
ISO 7000, 2609 Unsteril
Indica che il
dispositivo medico
non è stato sottoposto
a un processo di
sterilizzazione.
EN ISO 15223-1,
Allegato B
Prodotto privo di
lattice di gomma
naturale
Indica l’assenza di
gomma naturale secca
o di lattice di gomma
naturale.
ISO 7000, 2794 Unità di imbal-
laggio
Indica il numero di
pezzi contenuti nella
confezione.
FDA 21 CFR 801 Solo dietro pre-
scrizione medica
Attenzione: La legge
Federale Statunitense
limita la vedita di
questo depositivo
preparazione o su
prescrizione degli
stessi.
IEC 60417, 5140 Radiazioni elet-
tromagnet-iche
non ionizzanti
Indica livelli
generalmente elevati
e potenzialmente
pericolosi
di radiazioni non
ionizzanti, oppure
indica la presenza di
apparecchiature o
sistemi ad es. nell’area
elettromedicale, che
includono trasmettitori
RF o che applicano
intenzionalmente
energia
elettromagnetica RF
a scopo diagnostico o
terapeutico.
Simbolo Riferimento
standard e
numero simbolo
Denominazione
simbolo Descrizione simbolo
EN ISO 15223-1,
5.1.7
ISO 7000, 2498
Numero di serie
Indica il numero di
serie del produttore
per l’identificazione del
dispositivo medico.
ISO/DIS 15223-1,
5.7.11
ISO 7000, 3707
Sistema barriera
sterile monouso
Indica un sistema
barriera sterile
monouso.
EN ISO 15223-1,
5.2.3
ISO 7000, 2501
Sterilizzato con
ossido di etilene
Indica che il dispositivo
medico è stato
sterilizzato con ossido
di etilene.
EN ISO 15223-1,
5.3.7
ISO 7000, 0632
Limiti di tempe-
ratura
Indica i valori limite di
temperatura ai quali
il dispositivo medico
può essere esposto in
modo sicuro.
ISO 7000, 0623
ISO 780, 0623
IATA 2004
Questo lato verso
l’alto
Indica l’orientamento
verticale corretto della
confezione durante il
trasporto.
UDI
ISO/DIS 15223-1,
5.7.10
Identificativo
univoco di dis-
positivo
Indica gli identificativi
del dispositivo e
gli identificativi
di produzione del
dispositivo medico.
EN ISO 15223-1,
5.1.4
ISO 7000, 2607
Data di scadenza
Indica la data dopo
la quale il dispositivo
medico non deve
essere utilizzato.
Hologic, NovaSure e i relativi loghi sono marchi registrati di Hologic, Inc.
e/o delle sue società affiliate negli Stati Uniti e/o in altripaesi.
Il sistema di ablazione endometriale NovaSure a impedenza è prodotto
edistribuito da Hologic, Inc.
© 2014-2022 Hologic, Inc.
-
 1
1
-
 2
2
-
 3
3
-
 4
4
-
 5
5
-
 6
6
-
 7
7
-
 8
8
-
 9
9
-
 10
10
-
 11
11
-
 12
12
-
 13
13
-
 14
14
-
 15
15
-
 16
16
-
 17
17
-
 18
18
-
 19
19
-
 20
20
-
 21
21
-
 22
22
-
 23
23
-
 24
24
-
 25
25
-
 26
26
-
 27
27
-
 28
28
-
 29
29
-
 30
30
-
 31
31
-
 32
32
-
 33
33
-
 34
34
-
 35
35
-
 36
36
-
 37
37
-
 38
38
-
 39
39
-
 40
40
-
 41
41
-
 42
42
-
 43
43
-
 44
44
-
 45
45
-
 46
46
-
 47
47
-
 48
48
-
 49
49
-
 50
50
-
 51
51
-
 52
52
-
 53
53
-
 54
54
-
 55
55
-
 56
56
-
 57
57
-
 58
58
-
 59
59
-
 60
60
-
 61
61
-
 62
62
-
 63
63
-
 64
64
-
 65
65
-
 66
66
-
 67
67
-
 68
68
-
 69
69
-
 70
70
-
 71
71
-
 72
72
-
 73
73
-
 74
74
-
 75
75
-
 76
76
-
 77
77
-
 78
78
-
 79
79
-
 80
80
-
 81
81
-
 82
82
-
 83
83
-
 84
84
-
 85
85
-
 86
86
-
 87
87
-
 88
88
-
 89
89
-
 90
90
-
 91
91
-
 92
92
-
 93
93
-
 94
94
-
 95
95
-
 96
96
-
 97
97
-
 98
98
-
 99
99
-
 100
100
-
 101
101
-
 102
102
-
 103
103
-
 104
104
-
 105
105
-
 106
106
-
 107
107
-
 108
108
-
 109
109
-
 110
110
-
 111
111
-
 112
112
-
 113
113
-
 114
114
-
 115
115
-
 116
116
-
 117
117
-
 118
118
-
 119
119
-
 120
120
-
 121
121
-
 122
122
-
 123
123
-
 124
124
-
 125
125
-
 126
126
-
 127
127
-
 128
128
-
 129
129
-
 130
130
-
 131
131
-
 132
132
-
 133
133
-
 134
134
-
 135
135
-
 136
136
-
 137
137
-
 138
138
-
 139
139











































































































































in andere talen
- italiano: Hologic NovaSure Istruzioni per l'uso
- français: Hologic NovaSure Mode d'emploi
- Deutsch: Hologic NovaSure Bedienungsanleitung
Gerelateerde papieren
-
 Hologic NovaSure Handleiding
Hologic NovaSure Handleiding
-
 Hologic Aquilex Fluid Control System Handleiding
Hologic Aquilex Fluid Control System Handleiding
-
 Hologic Aquilex Fluid Management System Handleiding
Hologic Aquilex Fluid Management System Handleiding
-
 Hologic CoolSeal Generator Gebruikershandleiding
Hologic CoolSeal Generator Gebruikershandleiding
-
 Hologic CoolSeal Generator Gebruikershandleiding
Hologic CoolSeal Generator Gebruikershandleiding
-
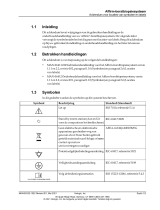 Hologic Affirm Breast Biopsy Guidance System Gebruikershandleiding
Hologic Affirm Breast Biopsy Guidance System Gebruikershandleiding
-
 Hologic Omni Instrument Tray Handleiding
Hologic Omni Instrument Tray Handleiding
-
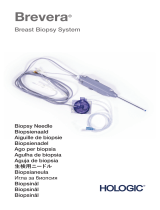 Hologic Brevera Breast Biopsy System Biopsy Needle Handleiding
Hologic Brevera Breast Biopsy System Biopsy Needle Handleiding
-
 Hologic ThinPrep 2000 Processor de handleiding
Hologic ThinPrep 2000 Processor de handleiding









Andere documenten
-
ResMed AirMini mount system Gebruikershandleiding
-
 Steris Sterile Water For Injection Handleiding
Steris Sterile Water For Injection Handleiding
-
 Johnson & Johnson Biosense Webster ThermoCool SmartTouch Instructions For Use Manual
Johnson & Johnson Biosense Webster ThermoCool SmartTouch Instructions For Use Manual
-
Enraf-Nonius NN ELEKTR. T.B.V. 3444.652 Handleiding
-
 Steris Lariat Snare Handleiding
Steris Lariat Snare Handleiding
-
-
-
 SCS Sentinel 3513143550068 de handleiding
SCS Sentinel 3513143550068 de handleiding



